
Nuclear medicine accuracy for early cancer detection depends on radiotracer specificity, equipment calibration, and physician expertise. AERB licensing and multidisciplinary review protocols separate diagnostic-grade facilities from commodity scan centers.
Key Takeaways
- Accuracy hinges on tracer-cancer matching: FDG-PET for most solid tumors, PSMA-PET for prostate cancer, DOTA-PET for neuroendocrine malignancies.
- AERB licensing confirms radiation safety protocols and tracer quality standards — verify your center appears on the May 2026 registry.
- Digital PET-CT scanners deliver higher spatial resolution than legacy analog systems, improving detection of sub-centimeter lesions.
- Multidisciplinary tumor board review reduces false-positive rates by integrating PET findings with pathology, serology, and clinical staging.
- Preparation steps — fasting, glucose control, hydration — directly affect tracer distribution and image clarity for accurate interpretation.
What Determines Nuclear Medicine Accuracy in Early Cancer Detection
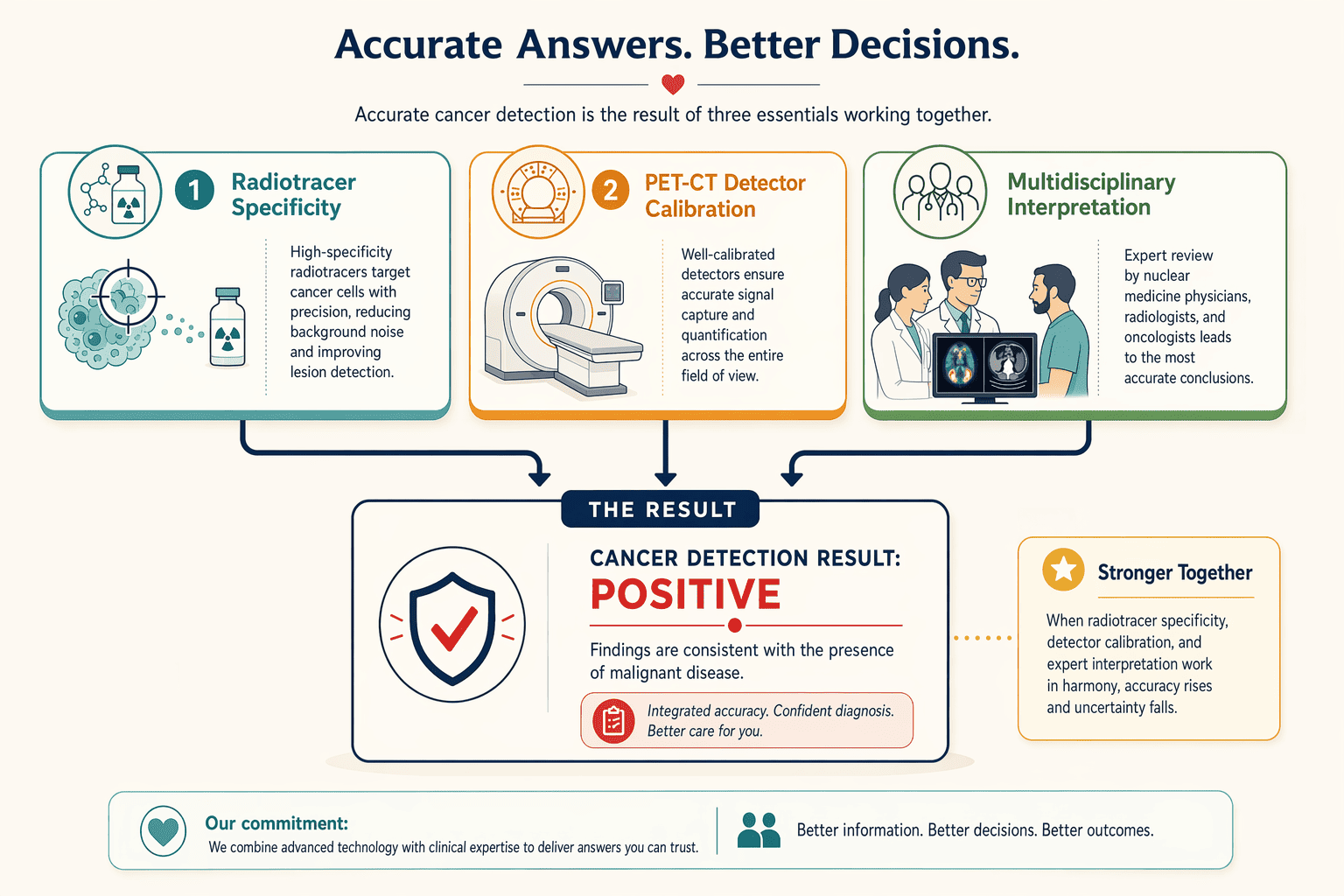
Accuracy in nuclear medicine depends on three interdependent factors: the radiotracer's biological specificity for the suspected cancer type, the PET-CT scanner's detector resolution and calibration protocols, and the interpretation framework — whether scans are reviewed by a single physician or a multidisciplinary tumor board. No facility brand alone guarantees accuracy; rather, the match between tracer selection, equipment standards, and collaborative review determines how reliably early-stage lesions are detected.
Tracer Specificity and Cancer-Type Sensitivity
Different radiotracers target distinct metabolic pathways, and sensitivity varies by cancer biology. 18F-FDG (fluorodeoxyglucose) exploits elevated glucose metabolism in most solid tumors — areas of higher metabolic activity exhibit increased tracer uptake, appearing as brighter spots on images. FDG remains the workhorse for staging lung, breast, and colorectal cancers, but its utility drops in slow-growing or glucose-independent malignancies. For prostate cancer, gallium-68 PSMA (prostate-specific membrane antigen) tracers bind to cell-surface receptors, achieving higher specificity than FDG. Similarly, DOTA-peptides image neuroendocrine tumors by targeting somatostatin receptors. A facility offering only FDG scans will miss cancers that require PSMA or DOTA imaging, tracer availability directly shapes diagnostic reach. Multi-tracer PET-CT centers address this limitation by maintaining multiple radiopharmaceuticals for organ-specific protocols.
Equipment Calibration and Detector Technology
Modern digital PET-CT scanners differ from legacy analog systems in spatial resolution and count-rate performance. Time-of-flight (TOF) detectors localize positron annihilation events with sub-centimeter precision, reducing false negatives in small (<1 cm) lesions. Yet hardware alone does not ensure accuracy, daily quality assurance checks verify detector uniformity, energy calibration, and timing alignment. Facilities that skip routine calibration protocols risk systematic errors: miscalibrated detectors can under-report tracer uptake, masking early-stage disease. For example, Andromeda Cancer Hospital operates a GE Discovery IQ 2 system, a TOF-capable platform, but accuracy hinges on adherence to manufacturer-specified QA workflows and periodic phantom imaging to confirm resolution benchmarks. Equipment generation matters less than calibration discipline when comparing AERB-licensed facilities.
Multidisciplinary Interpretation Protocols
Solo reads by nuclear medicine physicians produce lower diagnostic accuracy than multidisciplinary tumor-board reviews that integrate PET findings with pathology, serology, and clinical staging. A board comprising medical oncologists, radiation oncologists, radiologists, and nuclear medicine specialists cross-validates scan interpretation against other diagnostic modalities, flagging borderline uptake patterns that might be dismissed in isolation. This collaborative protocol reduces false positives (inflammatory uptake misread as malignancy) and false negatives (subtle lesions overlooked on single-specialty review). Facilities that embed PET-CT reporting within weekly tumor boards, rather than issuing standalone radiology reports, achieve higher concordance with surgical pathology outcomes. When evaluating centers, ask whether scan interpretation is performed solo or within a multidisciplinary conference that includes surgical and medical oncology input.
Understanding tracer specificity reveals why sensitivity and specificity metrics matter more than scanner brand when evaluating PET-CT centers.
How Pet-Ct Scans Detect Cancer Early: the Science Behind Sensitivity and Specificity
Sensitivity Vs Specificity in Cancer Imaging
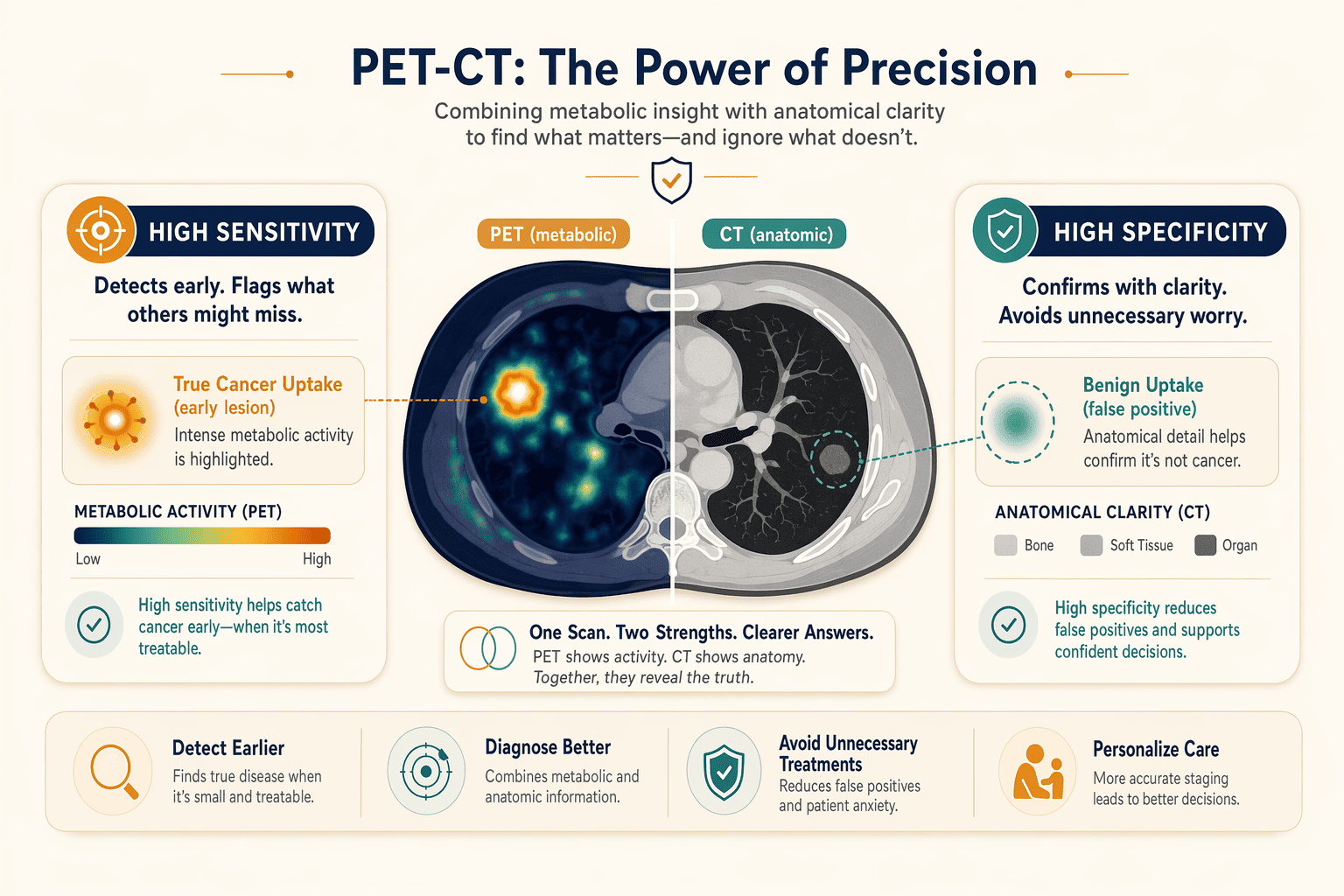
Positron emission tomography (PET) scans detect early signs of cancer by measuring metabolic activity in tissues. A PET scan often can find changes earlier than CT or MRI scans, which makes sensitivity, the test's ability to correctly identify true cancer cases, a critical measure. A scan with 90% sensitivity detects 90 of 100 actual cancers. However, high sensitivity can increase false positives: benign conditions that mimic cancer uptake may trigger alerts in healthy tissue. Specificity, the test's ability to correctly rule out cancer in disease-free patients, balances this trade-off. When PET is combined with CT, the resulting PET-CT scan gives more complete and more accurate information than either test alone, improving specificity by adding anatomical context to metabolic signals.
False-Positive and False-Negative Patterns
Inflammation, infection, and recent surgery can cause false-positive FDG uptake because activated immune cells consume glucose at elevated rates. Post-operative granulation tissue and autoimmune disease also mimic malignant metabolic patterns. Conversely, small tumors below the scanner's spatial resolution or slow-growing cancers with low glucose metabolism may yield false negatives. Radiologists differentiate true lesions from artifacts by correlating PET hotspots with CT anatomy, reviewing clinical history, and applying standardized uptake value (SUV) thresholds. Multi-phase imaging and delayed scans further refine accuracy by revealing how tracer uptake evolves over time.
Patient Preparation Protocols That Impact Scan Quality
Proper preparation directly affects FDG distribution and image clarity. Key steps include:
- Fasting for 4 to 6 hours before the scan to stabilize blood glucose and maximize tracer uptake in cancer cells.
- Blood glucose level check to ensure levels are below 200 mg/dL; elevated glucose competes with FDG, reducing scan sensitivity.
- Hydration protocol (water intake encouraged) to support tracer clearance from kidneys and bladder.
- Avoiding strenuous exercise 24 hours prior, as muscle activity increases FDG uptake in non-target tissue, creating confounding hotspots.
At Andromeda Cancer Hospital, PET-CT is an outpatient procedure with same-day or next-day reporting, and patients receive detailed prep instructions to optimize scan accuracy.
Scan accuracy depends not only on the science of radiotracer uptake but also on regulatory oversight that enforces quality standards across India's nuclear medicine facilities.
AERB Licensing and Quality Standards for Nuclear Medicine Facilities in India
The Atomic Energy Regulatory Board (AERB) is India's regulatory authority for radiation safety in nuclear medicine. Every PET-CT center must hold a valid AERB license to legally operate, the List of PET-CT Centres licensed by AERB (as on May 20, 2026) serves as the authoritative registry patients should consult before booking a scan. AERB licensing directly affects scan accuracy: licensed centers must meet technical standards for tracer quality control, dose calibration, shielding design, and personnel qualifications that unlicensed facilities bypass.
What AERB Licensing Requires From Pet-Ct Centers
AERB licensing enforces radiation safety protocols that directly impact scan reliability. Regulatory requirements for designing PET-CT facilities mandate structural shielding to protect patients and staff, calibrated dose calibrators to ensure tracer activity measurements remain precise, and sterile tracer sourcing with documented purity logs. Centers must employ AERB-certified Radiation Safety Officers (RSOs), for example, qualified RSO II and RSO III personnel oversee NM therapy compliance, who supervise quality control protocols including daily equipment checks, quarterly shielding audits, and radioactive waste disposal procedures.
Personnel qualifications matter: nuclear medicine physicians at licensed centers must hold recognized board certifications and complete radiation protection training aligned with IAEA standards for patient dose optimization. The tracer injection room, scanner suite, and uptake areas require AERB-approved lead shielding and ventilation systems to minimize radiation exposure. Dose calibrators must undergo annual calibration audits traceable to national standards, a lapsed calibration certificate means tracer activity errors that produce false-negative scans. Facilities that skip AERB licensing skip these checks entirely, leaving patients with no assurance that the injected tracer dose is accurate or that image reconstruction protocols follow evidence-based guidelines.
How to Verify a Facility's AERB Certification
Verification is straightforward: download the List of PET-CT Centres licensed by AERB (as on May 20, 2026) from the AERB website and search for the facility name, city, and state. The registry lists hundreds of centers, from Army Hospital R&R in New Delhi to ALL INDIA INSTITUTE OF MEDICAL SCIENCES BHUBANESWAR in Khordha, Orissa, and updates periodically to reflect newly licensed sites and suspended permits. If a center is absent from the registry, it operates without regulatory oversight of tracer quality, equipment calibration, or radiation protection.
The license number itself signifies quality compliance: centers must renew certification annually and pass unannounced AERB inspections that audit shielding integrity, dose calibrator performance, and personnel training records. A valid license means the facility has maintained calibrated scanners, sterile tracer handling, and documented quality control logs that trace back to regulatory audits. A lapsed or missing license means none of these safeguards apply, tracer purity may degrade undetected, dose calibrators may drift out of spec, and image reconstruction algorithms may lack physicist oversight. Before scheduling a PET-CT scan, verify the facility appears on the May 2026 AERB registry; centers not listed should be avoided regardless of how advanced their marketing claims appear.
Armed with knowledge of AERB standards and tracer biology, patients can apply four practical criteria to evaluate any PET-CT center before booking a scan.
What to Look for When Choosing a Pet-Ct Center for Cancer Screening
When evaluating a nuclear medicine facility for early cancer detection, four core criteria separate diagnostic-grade centers from commodity scan shops: regulatory licensing, tracer portfolio breadth, multidisciplinary review pathways, and equipment technology generation.
AERB Certification and Tracer Portfolio
Verify that the center holds current AERB (Atomic Energy Regulatory Board) licensing, this credential confirms that radiation safety officers meet national nuclear medicine standards. Beyond licensing, ask whether the facility stocks cancer-type-specific tracers. Generic FDG covers most solid tumors, but prostate cancer staging requires Ga-68 PSMA, neuroendocrine tumors benefit from DOTA peptides, and emerging FAPI tracers improve lung cancer detection. A center offering only FDG may force you to seek a second scan elsewhere when molecular profiling demands a targeted tracer.
Multidisciplinary Tumor Board Access
Ask whether scan reports route to a tumor board where medical oncologists, surgical oncologists, radiologists, and nuclear medicine physicians review findings together. Single-physician interpretation increases the risk that subtle metabolic patterns are missed, collaborative review correlates with higher diagnostic confidence and fewer false positives, particularly in borderline staging scenarios.
Equipment Technology and Reporting Turnaround
Digital PET-CT scanners, introduced in South Asia in 2019, deliver higher spatial resolution and faster acquisition than analog systems, reducing both scan time and radiation exposure. Confirm the detector technology (digital detectors with time-of-flight capability outperform older photomultiplier tubes) and ask about routine quality-assurance protocols. Finally, verify reporting timelines: same-day or next-day reads are standard for urgent staging, while multi-day delays may indicate understaffing or equipment bottlenecks. PET-CT fusion, combining metabolic and anatomical imaging, is the recognized standard; standalone PET without CT co-registration is outdated for cancer screening.
Andromeda Cancer Hospital's Nuclear Medicine and Pet-Ct Services
Pet-Ct Technology and Tracer Availability at Andromeda
Andromeda Cancer Hospital provides whole-body PET-CT scans as an outpatient procedure, allowing patients to return home the same day. The facility offers a range of specialized PET-CT scans tailored to detect specific cancer types with high accuracy, supporting early detection, accurate staging, treatment planning, response assessment, and follow-up monitoring. These capabilities align directly with the multidisciplinary diagnostic framework outlined in earlier sections, where tracer specificity and image quality determine how early abnormalities appear on a scan.
Andromeda's tracer portfolio includes standard FDG-PEThttps://andromedahospital.in/treatments/nuclear-medicine-pet-ct for glucose metabolism imaging alongside advanced options for prostate, neuroendocrine, and other malignancies. This breadth mirrors offerings at regional competitors such as Sarvodaya Cancer Institute, which lists FDG, Ga-68 PSMA, DOTA, FAPI, and additional specialized tracers on its PET-CT page. While Mahajan Imaging emphasizes digital PET-CT with high-resolution lesion detection and minimal radiation exposure, and Yashoda Hospital positions PET-CT within a thorough diagnostic lab infrastructure, all three facilities, like Andromeda, operate under AERB licensing and publish same-day or next-day reporting workflows.
Multidisciplinary Oncology Team and Reporting Workflow
Accuracy in nuclear medicine extends beyond scanner specifications to the physician collaboration model. At Andromeda Cancer Hospital, nuclear medicine physicians participate in weekly tumor board reviews alongside surgical oncologists, medical oncologists, radiation oncologists, and pathologists. This multidisciplinary structure ensures that PET-CT findings inform surgical margins, chemotherapy regimens, and radiation field planning in real time, a practice that reduces missed lesions and prevents under-staging.
One anonymized case illustrates the impact: a patient with suspected localized breast cancer underwent preoperative PET-CT at Andromeda; the scan revealed unexpected axillary and mediastinal uptake. During tumor board discussion, the surgical team deferred immediate mastectomy, the medical oncology team initiated neoadjuvant chemotherapy, and a repeat PET-CT six weeks later confirmed downstaging, ultimately allowing breast-conserving surgery. Without cross-specialty review, the initial surgical plan would have proceeded based on CT and ultrasound alone, missing distant nodal involvement until post-operative pathology.
Cost, Insurance Coverage, and Patient Preparation
PET-CT remains a high-cost procedure in India, with scan fees typically ranging from ₹18,000 to ₹35,000 depending on tracer type and facility location. Insurance coverage varies by policy and cancer indication; many public and private insurers approve FDG-PET for confirmed malignancies but may deny coverage for screening or non-oncologic applications. Patients at Andromeda Cancer Hospital are advised to verify policy eligibility before booking, as out-of-pocket expenses can exceed ₹25,000 for specialized tracers like Ga-68 PSMA or FAPI.
Preparation protocols include fasting for four to six hours before FDG-PET scans to minimize background glucose uptake, and avoidance of strenuous exercise the day prior. Diabetic patients receive specific glucose-control instructions to prevent false-negative results. Breastfeeding mothers are typically advised to suspend nursing for 12 to 24 hours post-injection, depending on the radiotracer's half-life, to minimize infant exposure, a precaution Andromeda's nuclear medicine team discusses during pre-scan consultations. These requirements, while standard across AERB-licensed centers, can complicate scheduling for patients managing comorbidities or caregiving responsibilities.
Strengths
- Whole-body PET-CT capability supporting early detection and accurate staging across multiple cancer types
- Outpatient procedure model with same-day discharge, reducing hospitalization burden
- Integrated multidisciplinary tumor board workflow, nuclear medicine physicians collaborate directly with surgical, medical, and radiation oncology teams
- Thorough cancer care under one roof, enabling smooth coordination from imaging through treatment delivery
Limitations
- High out-of-pocket cost (₹18,000, ₹35,000 per scan) with variable insurance coverage, particularly for specialized tracers or non-curative indications
- Fasting and preparation protocols may complicate scheduling for diabetic patients or those with tight caregiving responsibilities
- Breastfeeding suspension periods (12 to 24 hours post-injection) require advance planning for nursing mothers
- Public data on specific tracer availability beyond FDG not disclosed on hospital website, requiring direct inquiry for prostate or neuroendocrine cancer patients
Best For
Andromeda Cancer Hospital's PET-CT service is best suited for patients seeking thorough oncology care within a single institution where nuclear medicine findings directly inform surgical and systemic treatment decisions through weekly tumor board review. The outpatient model appeals to those who prefer same-day discharge, and the facility's location in Sonipat, near the Delhi border with road connectivity to NCR, serves patients across Haryana, Punjab, and western Uttar Pradesh. However, individuals prioritizing lowest-cost imaging or those requiring immediate confirmation of specialized tracer availability (PSMA, FAPI, DOTA) may benefit from comparing pricing and tracer menus across Andromeda, Sarvodaya, Mahajan, and Yashoda before booking.
Conclusion
Cost-focused PET-CT centers may offer lower prices but lack multi-tracer portfolios or tumor board review, Andromeda and similar thorough cancer hospitals integrate PET-CT into multidisciplinary oncology workflows but at higher cost. Standalone imaging centers deliver faster reporting turnaround (24-48 hours) for routine scans, while hospital-based nuclear medicine departments route complex cases to tumor boards, adding 2-3 days but improving diagnostic confidence for ambiguous findings.
As digital PET-CT technology becomes standard across India and AERB expands licensing oversight, the gap between high-quality and low-quality nuclear medicine facilities will narrow, but multidisciplinary tumor board access and cancer-type-specific tracer expertise will remain the differentiators for early cancer detection accuracy through 2027 and beyond.
Verify your chosen PET-CT center's AERB licensing status using the May 2026 registry, confirm they offer the tracer matched to your cancer-screening need, and explore Andromeda Cancer Hospital's nuclear medicine services if you want whole-body PET-CT integrated with multidisciplinary oncology care in Delhi NCR.
Frequently Asked Questions
What is the most accurate PET scan for cancer detection?
The most accurate PET scan depends on cancer type: FDG-PET for most solid tumors exploiting elevated glucose metabolism, PSMA-PET for prostate cancer, and DOTA-PET for neuroendocrine tumors. Tracer-cancer specificity drives sensitivity, so matching the radiotracer to the suspected malignancy is key.
How do I know if a PET-CT center is AERB-licensed?
Check the AERB PET-CT registry (May 2026 PDF) for the center's name and license number. AERB licensing ensures radiation safety officers meet national nuclear medicine standards and tracer quality protocols are enforced. Only licensed centers legally operate PET-CT equipment in India.
Can a PET scan detect cancer before symptoms appear?
Yes, PET scans measure metabolic activity and often detect cancer before anatomical changes appear on CT or MRI. However, sensitivity depends on tumor size and tracer uptake, very small lesions or low-metabolism cancers may not produce sufficient signal for early detection.
What causes false-positive results on a PET scan?
False-positive FDG uptake occurs in inflammation, infection, recent surgery, and autoimmune disease because activated immune cells consume glucose at elevated rates. Nuclear medicine physicians differentiate these patterns from malignancy by cross-referencing CT anatomy, patient history, and clinical findings.
Does Andromeda Cancer Hospital offer whole-body PET-CT scans?
Yes, Andromeda Cancer Hospital provides whole-body PET-CT scans as an outpatient procedure for cancer staging, metastasis detection, and post-treatment follow-up. The service includes specific preparation protocols to optimize tracer distribution and image clarity for accurate diagnostic interpretation.
How long does it take to get PET scan results?
Routine scans typically yield results in 24-48 hours. Centers using multidisciplinary tumor board review, where medical oncologists, radiologists, and nuclear medicine physicians integrate PET findings with pathology and serology, may require 2-3 additional days but deliver higher diagnostic confidence.
Is PET-CT covered by insurance in India?
Coverage varies by policy and cancer type. Many public and private insurers approve FDG-PET for confirmed malignancies but may deny claims for screening in asymptomatic patients. Verify eligibility with your insurer before scheduling to avoid unexpected out-of-pocket costs ranging ₹18,000-₹35,000.
Sources
- 18F-FDG PET/CT Imaging In Oncology - PMC - pmc.ncbi.nlm.nih.gov
- PET Scanning - StatPearls - NCBI Bookshelf - www.ncbi.nlm.nih.gov
- PET Scan: Procedure Details and Results - Cleveland Clinic - my.clevelandclinic.org
- Positron emission tomography (PET) scan - Mayo Clinic - www.mayoclinic.org
- List of PET-CT Centres licensed by AERB (as on May 20, 2026) - www.aerb.gov.in (2026)
- Regulatory requirements for designing PET-CT facility in India - PMC - pmc.ncbi.nlm.nih.gov
- Radiation protection of patients during PET/CT scanning - www.iaea.org