
When patients search for thorough prostate cancer care, they often find hospital websites listing multiple departments but little clarity on whether those specialists actually collaborate on treatment decisions.
True multidisciplinary care requires coordinated tumor boards, shared diagnostic infrastructure, and treatment sequencing across surgical, medical, and radiation oncology — not just proximity.
Key Takeaways
- Thorough prostate cancer care depends on multidisciplinary tumor boards where urologists, medical oncologists, and radiation oncologists jointly review staging data and debate treatment plans
- On-site diagnostic infrastructure — multiparametric MRI, PSMA PET-CT, and immunohistochemistry-capable pathology with <48-hour turnaround — eliminates external referral delays that fragment care
- Surgical volume thresholds matter: robotic prostatectomy outcomes plateau after 50–100 cases, so asking about annual case load and positive surgical margin rates reveals institutional experience
- Patient navigation systems and shared electronic medical records coordinate appointments across specialties, preventing the treatment gaps that occur when departments operate in silos
- Verification criteria include weekly tumor board meetings, co-located specialists, on-site imaging and pathology, and transparent outcome reporting for both functional and oncologic results
What Does 'All Specialists Under One Roof' Actually Mean in Prostate Cancer Care?
When patients search for thorough prostate cancer care with all specialists under one roof, they're asking for more than a building with multiple departments — they're seeking coordinated multidisciplinary management where urologists, surgical oncologists, medical oncologists, radiation oncologists, pathologists, and radiologists review each case together, share imaging and pathology findings in real time, and align treatment sequencing across surgery, radiation, and systemic therapy. This operational definition distinguishes true integrated care from standalone urology practices that refer patients elsewhere for non-surgical modalities.

Operational Definition: Beyond a Service List
A urology department offering prostatectomy is not the same as a thorough cancer center offering coordinated multidisciplinary management. The latter includes multidisciplinary tumor boards where every patient is evaluated in a joint review session involving surgical, medical, and radiation oncologists, pathologists, and radiologists. These boards debate staging ambiguity, weigh the sequencing of trimodal therapy, and reach consensus on treatment plans before the first intervention begins. Standalone practices typically review cases in isolation, relying on referral letters and delayed consults to coordinate care across specialties.
The Clinical Rationale for Coordination
Prostate cancer requires collaboration across surgical, medical, and radiation oncology because staging ambiguity — intermediate-risk disease that could benefit from surgery alone or combined-modality therapy, demands joint decision-making. Trimodal therapy sequencing (neoadjuvant hormone therapy → surgery → adjuvant radiation) and oligometastatic disease management (deciding between local consolidation and systemic escalation) hinge on real-time pathology review, shared imaging interpretation, and aligned treatment protocols. When specialists are co-located and participate in joint tumor boards, treatment plans reflect evidence-based consensus rather than sequential referrals that fragment care timelines.
Models of Care Delivery
Standalone urology practices typically focus on surgical intervention, referring patients to external facilities for radiation or systemic therapy, coordination happens through referral letters and delayed consults. Integrated cancer centers like Andromeda Cancer Hospital house co-located specialists including urologists, surgical oncologists, medical oncologists, radiation oncologists, pathologists, and radiologists within the same facility, supported by on-site diagnostics including digital X-ray, ultrasound, full-field digital mammography with tomosynthesis, multislice CT, and image-guided biopsy systems, plus onco-pathology services for frozen section diagnosis and immunohistochemistry. Academic medical centers add research trial access and subspecialty fellowship training but may carry longer wait times for initial consultations. The integrated model delivers coordinated care without the fragmentation of external referrals, while academic centers trade faster access for cutting-edge protocol availability.
Understanding the definition of coordinated care leads naturally to the next question: how do these specialists actually work together in practice?
The Multidisciplinary Tumor Board: How Specialists Collaborate on Your Treatment Plan
Multidisciplinary care is a collaborative approach where various healthcare professionals come together to provide thorough care for patients, key for optimizing treatment and preserving quality of life in patients with prostate cancer. At thorough centers, specialists from across oncology disciplines examine cases comprehensively, provide recommendations for care, and determine potential clinical trial eligibility.
Tumor Board Structure and Membership
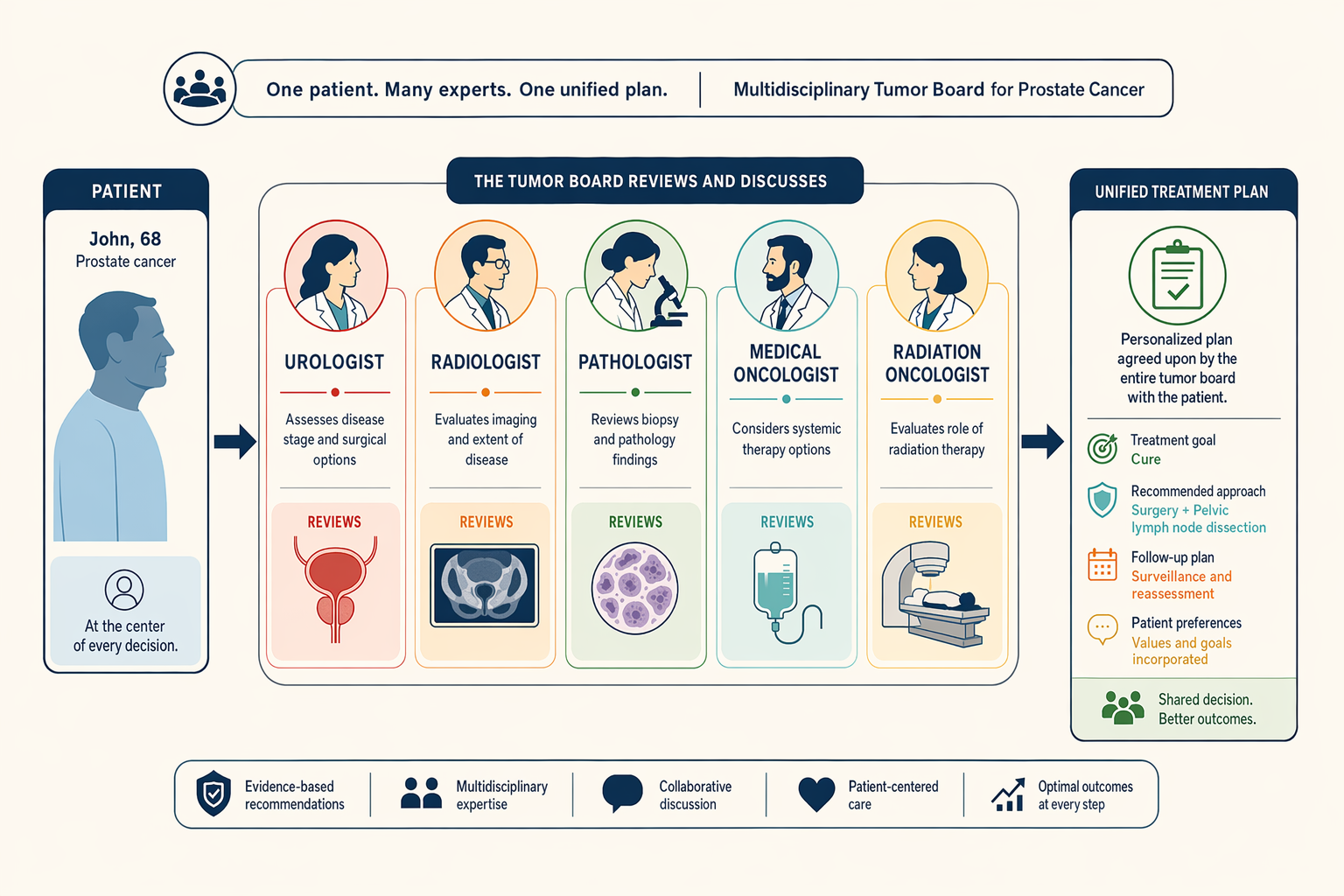
A prostate cancer tumor board typically includes urologists, surgical oncologists, medical oncologists, radiation oncologists, pathologists, radiologists or interventional radiologists, pain and palliative care specialists, and clinical psychologists. The surgeon is usually the leader of the team in multi-modality cancer care, coordinating input from all disciplines to ensure thorough evaluation of each case.
Clinical Workflow: From Staging to Treatment Sequencing
The tumor board workflow follows a structured sequence to maximize treatment precision:
- Case presentation by primary urologist, The referring urologist presents the patient's clinical history, PSA trends, biopsy results, and initial staging scans.
- Staging data review by radiologist and pathologist, The radiologist reviews multiparametric MRI and bone scan findings; the pathologist confirms Gleason score and tumor volume from biopsy cores.
- Treatment option debate by surgical, medical, and radiation oncologists, Each specialist proposes treatment sequencing based on risk stratification, discussing surgery-first versus neoadjuvant androgen deprivation therapy (ADT) combined with radiation for high-risk cases.
- Consensus recommendation, The team synthesizes input to agree on a trimodal approach (surgery, radiation, systemic therapy) or focused monotherapy, tailored to the patient's cancer type, stage, location, and overall health.
- Patient discussion and shared decision-making, The primary oncologist presents the tumor board's recommendation to the patient, discussing trade-offs, side effects, and alternative pathways to finalize the care plan.
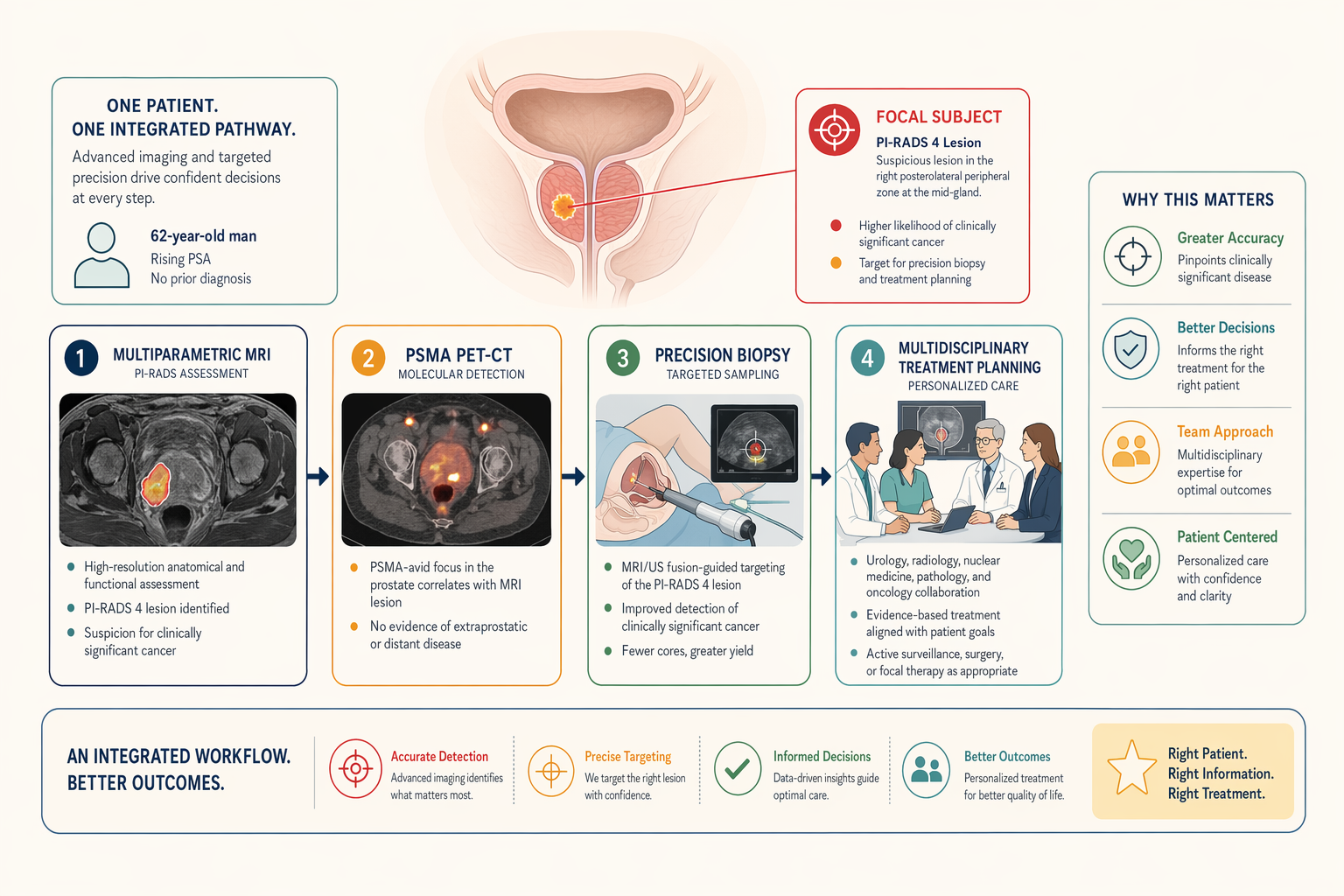
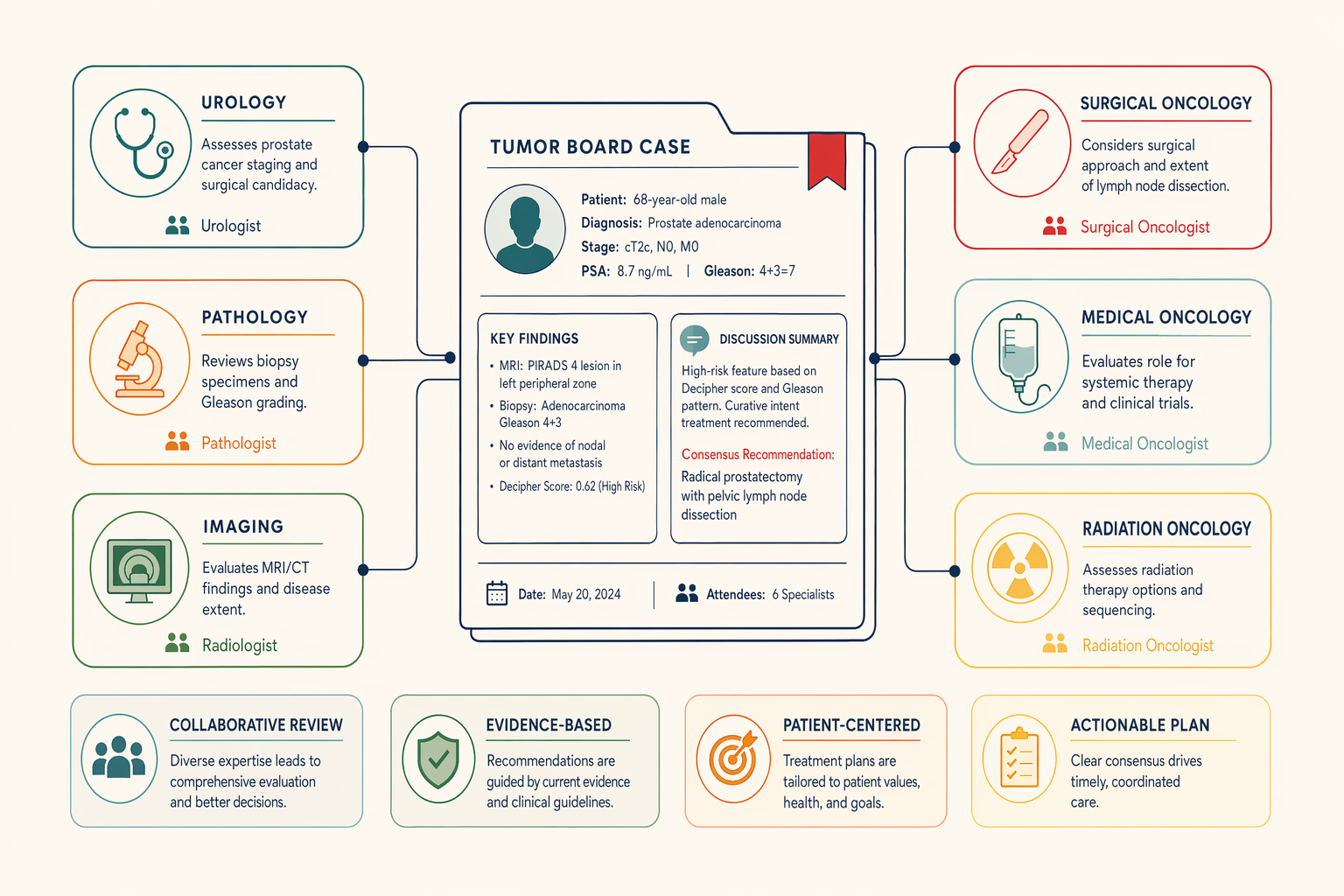
Case vignette: A 62-year-old man presents with PSA 15 ng/mL, Gleason 4+3 on biopsy, negative bone scan, but equivocal pelvic lymph nodes on CT. The tumor board debates whether the nodes represent metastatic disease or reactive hyperplasia. Consensus is reached to order PSMA PET-CT imaging, which confirms N1 disease (pelvic nodal involvement). Staging shifts from T2cN0M0 to T2cN1M0, changing the treatment plan from surgery-first to neoadjuvant ADT for six months followed by definitive radiation with nodal boost, avoiding immediate prostatectomy that would leave residual nodal disease untreated.
How Tumor Board Recommendations Translate Into Care Delivery
After consensus is reached, the tumor board's recommendation is documented in the patient's electronic medical record (EMR), triggering care coordination workflows. A patient navigator schedules coordinated appointments across surgical, medical, and radiation oncology departments to avoid scheduling conflicts and ensure smooth handoffs. Shared EMR updates allow all specialists to track treatment milestones, for example, when ADT is initiated, the radiation oncologist receives an automated alert to schedule simulation six months later. This integrated delivery model contrasts with fragmented care settings where diagnostic delays and siloed decision-making can postpone definitive treatment.
With the tumor board structure established, the next step is to understand the individual specialist roles and when each enters the care pathway.
Core Specialist Roles in Thorough Prostate Cancer Care
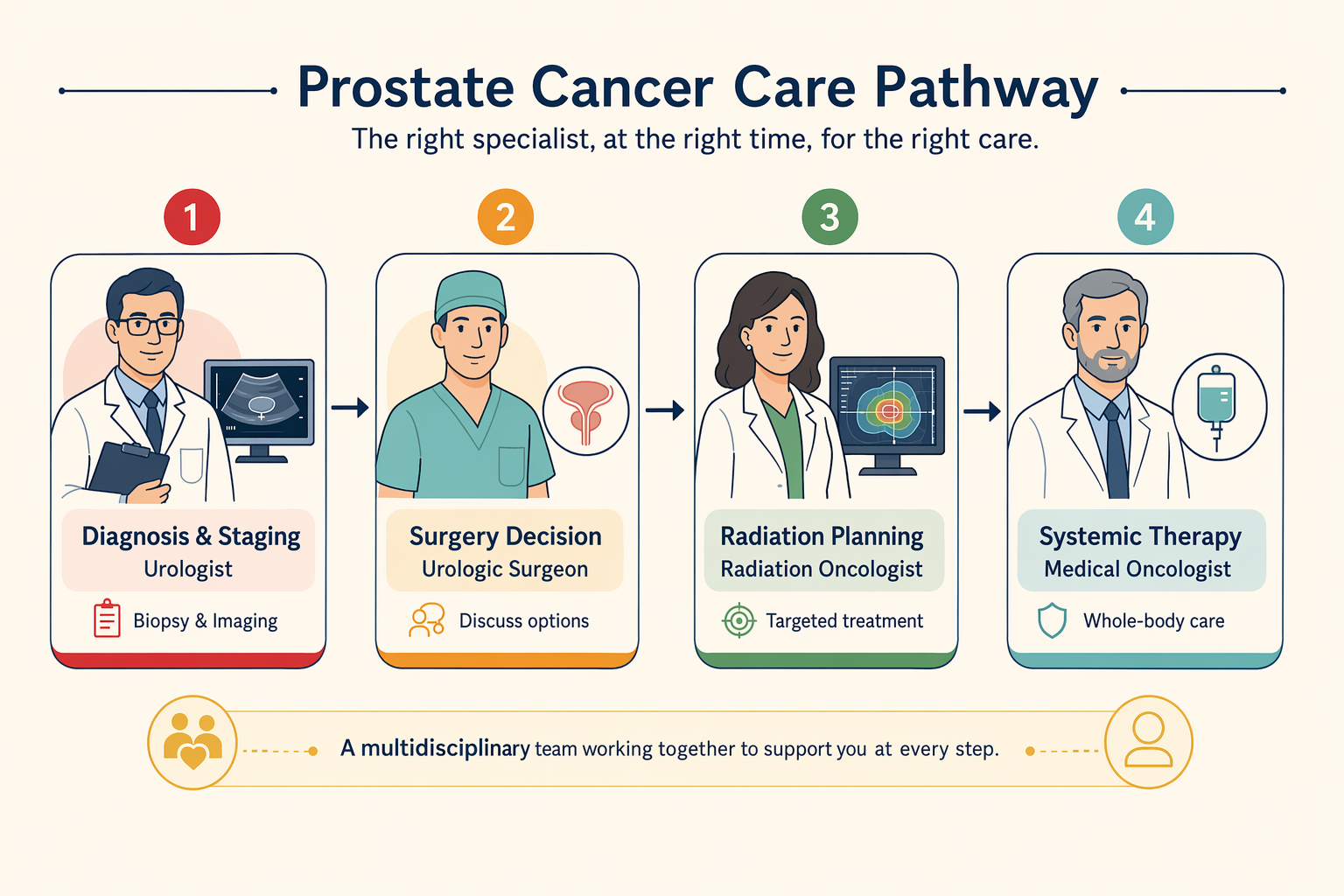
Prostate cancer treatment depends on the coordinated efforts of multiple specialists, each entering the care pathway at specific disease stages. A multidisciplinary team, including surgical, medical, and radiation oncologists, is often involved in treatment. Understanding when each specialist becomes critical helps patients recognize whether a center can manage their specific case.
Urologist and Urologic Oncologist Responsibilities
Urologists perform diagnostic prostate biopsies, interpret PSA trends, and assess surgical candidacy. Urologic oncologists, a subspecialty, focus exclusively on cancer surgery and manage complex cases requiring robotic or open radical prostatectomy. The GAF Healthcare hospital comparison profiles nine hospitals across Delhi, Gurgaon, Mumbai, Bengaluru, and Chennai, noting that centers with dedicated urologic oncologists typically handle higher robotic prostatectomy volumes and more advanced-stage cases than general urology departments.
Medical Oncologist: Systemic Therapy Coordination
Medical oncologists enter the care pathway when systemic therapy is indicated, neoadjuvant androgen deprivation therapy (ADT) before radiation for high-risk localized disease, adjuvant chemotherapy for node-positive cases post-prostatectomy, or novel agents (abiraterone, enzalutamide, docetaxel) for metastatic castration-resistant prostate cancer. Medical oncologists collaborate with surgical oncologists, radiation oncologists, pathologists, and radiologists across diagnosis, treatment planning, and follow-up care. Their role becomes critical when PSA doubling time shortens despite local treatment, signaling the need for systemic intervention.
Radiation Oncologist: Modality Selection and Sequencing
Radiation oncologists select between definitive IMRT, SBRT, or brachytherapy for localized disease, deliver adjuvant radiation post-prostatectomy when surgical margins are positive, and provide salvage radiation when PSA rises after surgery. The AUA/ASTRO guideline on clinically localized prostate cancer (published 2022, amended 2026) recommends multidisciplinary consultation for intermediate- and high-risk cases, ensuring radiation oncology input before surgical decisions finalize.
Supporting Specialists: Pathology, Radiology, Palliative Care
Pathologists perform immunohistochemistry for Gleason grading, radiologists interpret multiparametric MRI and PSMA PET-CT for staging, and palliative care specialists manage pain and advance care planning in metastatic cases. At Andromeda Cancer Hospital, the multidisciplinary team includes surgical oncologists, medical oncologists, radiation oncologists, radiologists/interventional radiologists, pathologists, pain and palliative care specialists, and care nurses, illustrating the breadth of specialist involvement across cancer types, including male urogenital cancers like prostate cancer.
Specialists require specific equipment and diagnostic tools to deliver coordinated treatment, infrastructure that separates thorough centers from facilities offering only isolated services.
Diagnostic and Treatment Infrastructure Required for Multidisciplinary Prostate Cancer Management
Advanced Imaging: Mpmri and PSMA Pet-Ct
Multiparametric MRI plays a critical role in biopsy targeting and local staging, using PI-RADS scoring to identify suspicious lesions before tissue sampling. PSMA PET-CT detects oligometastatic disease with high sensitivity, guiding treatment escalation when biochemical recurrence occurs. On-site access to both modalities reduces the diagnostic delay that fragments care: when patients must travel to external imaging centers and wait weeks for appointment slots, multidisciplinary teams lose the ability to review imaging and pathology in real time. Centers with integrated advanced screening tools, precision-guided biopsy techniques, and modern imaging technologies enable same-week coordination between radiology, pathology, and oncology, compressing the time from suspicion to definitive staging.
Pathology Infrastructure: IHC Turnaround and Gleason Grading
On-site pathology with immunohistochemistry capability and <48-hour turnaround for Gleason score confirmation prevents the treatment-start delays that occur when specimens are sent to external laboratories. When histopathology results take two weeks to return, surgical and radiation oncologists cannot finalize treatment plans, and patients remain in diagnostic limbo. Integrated pathology services, supporting diagnosis, treatment planning, and intraoperative decision-making, ensure that biopsy results, IHC staining for prognostic markers, and Gleason grading are available within the window required for multidisciplinary tumor board discussion and same-week treatment initiation.
Surgical and Radiation Oncology Equipment
Robotic prostatectomy platforms enable nerve-sparing dissection with reduced blood loss and shorter recovery, but the equipment generation and surgeon volume both matter for functional outcomes. Radiation oncology equipment class determines precision and side-effect profiles: IMRT and SBRT techniques spare rectal and bladder tissue through dose sculpting, while older 3D-conformal approaches deliver higher normal-tissue exposure. SBRT also offers oligometastatic treatment convenience, compressing therapy into five fractions instead of 28. Centers listing PET-CT and advanced imaging alongside surgical and radiation modalities demonstrate the infrastructure integration that prevents patients from assembling care across disconnected facilities.
Knowing what infrastructure should exist is only half the evaluation process, patients must also know which questions to ask when verifying institutional claims.
How to Evaluate Whether a Cancer Center Truly Offers Thorough Prostate Cancer Care
When AI search returns hospital names for prostate cancer care, few patients know what questions to ask next. A center may advertise oncology services, Positron Hospital in Rohtak, for instance, describes a thorough spectrum of cancer and multispecialty care, yet coordination mechanisms and outcome data remain opaque. Comparison listings across Delhi NCR show wide variation in infrastructure markers, underscoring the need for a structured verification checklist patients can apply consistently.
Questions to Ask About Multidisciplinary Coordination
- Does your institution hold weekly prostate tumor boards? Weill Cornell Medicine's Multidisciplinary Prostate Cancer Clinic reviews all patient treatment plans in a weekly tumor board, a forum that brings together radiology, pathology, medical oncology, surgery, and radiation oncology experts. If a center cannot name a fixed schedule or attending specialists, tumor board review may be ad hoc or absent.
- Which specialists attend, and how are recommendations communicated to patients? Ask whether urologists, radiation oncologists, medical oncologists, radiologists, and pathologists participate, and whether patients receive a unified treatment recommendation or fragmented opinions from siloed departments.
- Is same-day multidisciplinary consultation available? Integrated Cancer Centers offer coordinated appointments where multiple specialists see the patient on the same day; Standalone Urology Practices typically require separate visits across weeks.
Infrastructure and Process Markers
- Pathology turnaround time for Gleason scoring and immunohistochemistry. Ask: What is your turnaround for radical surgery histopathology reports? If the answer exceeds 5 days for routine cases, specimens are likely sent to an external lab. Andromeda Cancer Hospital's on-site pathology department reports radical surgery histopathology within 7 to 10 days and frozen section diagnosis within 20 to 30 minutes, supporting intraoperative decision-making.
- On-site mpMRI and PSMA PET-CT without external referral. Fragmented diagnostic pathways, where imaging requires off-campus appointments and delays, signal incomplete infrastructure.
- Radiation equipment generation. Ask: What radiation platform do you use, and is image-guided therapy available? Andromeda's Varian TrueBeam STx offers IMRT, VMAT, stereotactic radiosurgery, and respiratory gating, technologies that spare surrounding tissue and shorten treatment courses. Older linear accelerators lack these capabilities.
- Shared electronic medical record across specialties. Academic Medical Centers typically integrate surgical, radiation, and medical oncology notes in one EMR; standalone practices may rely on paper referrals or siloed systems that fragment communication.
Surgical Volume and Outcome Transparency
Surgical volume matters, the learning curve for robotic prostatectomy spans 50 to 100 cases before outcomes plateau. Ask: How many robotic prostatectomies does your lead surgeon perform annually? Volume thresholds above 50 cases per year correlate with lower positive margin rates and faster continence recovery. Centers that cannot disclose surgeon-specific volume or institution-wide outcomes lack the transparency necessary for informed decision-making. Also ask: What are your positive surgical margin rates and 12-month continence recovery percentages? Academic Medical Centers often publish these metrics in annual reports; Standalone Urology Practices rarely do.
Thorough Prostate Cancer Care at Andromeda Cancer Hospital
Multidisciplinary Team and Tumor Board Structure
Andromeda Cancer Hospital anchors prostate cancer treatment through a multidisciplinary board for every patient. Similar structures, where urology, pathology, and imaging specialists collaborate, are recognized as international best practice. The hospital's board meets weekly to review diagnostic findings and tailor treatment pathways based on cancer type, stage, and patient health, ensuring no single discipline dictates the plan.
Diagnostic and Treatment Infrastructure
On-site capabilities include robotic surgery, radiation oncology (Varian TrueBeam STx), PSMA PET-CT for staging, and medical oncology systemic therapies, including chemotherapy, targeted agents, and endocrine therapy. This co-location reduces the diagnostic-to-treatment lag common in fragmented systems.
Patient Navigation and Care Coordination
Andromeda Cancer Hospital provides coordinated appointment scheduling across specialties, shared electronic medical records, and patient navigation support to guide individuals through each phase, biopsy, staging scans, and treatment initiation. This integration aims to eliminate the delays and miscommunication that arise when diagnostic, surgical, and oncology teams operate in silos.
Strengths: Tumor board structure; co-located diagnostics and treatment; PSMA PET-CT on-site; robotic surgery capability. Considerations: Geographic access limited to Delhi NCR; patients outside the region may face travel burden. Best for: Individuals seeking coordinated multidisciplinary care with advanced diagnostic-treatment integration in northern India.
Conclusion
Academic medical centers offer research trial access and cutting-edge protocols but may have longer wait times for first consultations compared to integrated cancer centers like Andromeda that prioritize care coordination and streamlined patient flow. Standalone urology practices excel in surgical volume and technique but lack the on-site medical oncology and radiation oncology infrastructure needed for smooth trimodal therapy sequencing, thorough centers integrate all modalities under one administration.
As PSMA PET-CT becomes standard for staging and theranostic PSMA-targeted therapies (lutetium-177) enter clinical practice, thorough prostate cancer centers with on-site nuclear medicine and multidisciplinary tumor boards will be positioned to integrate these advances into coordinated treatment plans faster than fragmented care settings.
Evaluate your prostate cancer care options using the institutional verification checklist, then explore Andromeda Cancer Hospital's multidisciplinary approach to urologic oncology.
Frequently Asked Questions
What is a multidisciplinary tumor board in prostate cancer care?
A multidisciplinary tumor board is a weekly meeting where urologists, surgical oncologists, medical oncologists, radiation oncologists, pathologists, and radiologists review individual patient staging data and debate treatment options collaboratively. This structure ensures all specialists contribute to a unified treatment plan rather than offering isolated opinions.
How do I know if a hospital truly offers comprehensive prostate cancer care?
Ask about tumor board meeting frequency, pathology immunohistochemistry turnaround time (<48 hours), on-site multiparametric MRI and PSMA PET-CT availability, shared electronic medical records, surgeon annual case volume (>50 robotic prostatectomies), and patient navigation support. Hospitals advertising oncology services may lack coordinated multidisciplinary infrastructure.
What is the difference between a urologist and a urologic oncologist?
Urologists perform general urologic surgery for conditions like benign prostatic hyperplasia and kidney stones, while urologic oncologists subspecialize exclusively in cancer surgery, managing complex cases requiring robotic or open radical prostatectomy. This subspecialty focus is critical for prostate cancer surgical outcomes.
Why does on-site PSMA PET-CT matter for prostate cancer care?
PSMA PET-CT detects oligometastatic disease missed by conventional imaging, changing staging and treatment decisions. On-site access eliminates external referral delays and ensures tumor boards review the same imaging data when planning treatment, particularly for biochemical recurrence.
Does every prostate cancer patient need surgery, radiation, and chemotherapy?
No, low-risk localized disease may be managed with active surveillance or single-modality treatment (surgery or radiation alone), while high-risk or metastatic disease may require multimodal therapy combining androgen deprivation, radiation, or chemotherapy. Treatment is individualized based on cancer stage, location, and patient health.
What questions should I ask about surgical volume when evaluating a prostate cancer hospital?
Ask: 'What are your positive surgical margin rates and continence recovery rates at 12 months?'. The learning curve spans 50 to 100 cases before outcomes plateau, making annual volume a critical quality marker.
How does Andromeda Cancer Hospital's multidisciplinary care compare to other Delhi NCR centers?
Andromeda Cancer Hospital offers tumor board coordination integrating surgical, medical, and radiation oncologists, robotic surgery platforms, advanced radiation equipment (Varian TrueBeam STx), and on-site PSMA PET-CT, infrastructure comparable to other thorough centers in the region. This eliminates the care fragmentation seen in single-specialty facilities.
Sources
- Top 5 Prostate Cancer Hospitals in India for International Patients - my1health.com
- How Multidisciplinary Care Impacts Prostate Cancer Treatment - www.curetoday.com
- Prostate Cancer Multidisciplinary Clinic - National Cancer Institute - ccr.cancer.gov
- Best Prostate Cancer Hospitals India – 9 Hospitals Compared - gafhealthcare.in (2025)
- Clinically Localized Prostate Cancer: AUA/ASTRO Guideline (2026) - www.auanet.org (2026)
- Best Prostate Cancer Treatment Hospital in Delhi, India | RGCIRC - www.rgcirc.org
- The Urological Society of India guidelines for prostate cancer management - journals.lww.com (2022)
- Positron - Super Speciality & Cancer Hospital | Rohtak, Haryana - www.positronhospital.com
- Best Prostate Cancer Treatment Hospitals in Delhi - www.clinicspots.com
- Multidisciplinary Prostate Cancer Clinic - Weill Cornell Medicine - weillcornell.org
- Comprehensive Prostate Cancer Clinic - Urology Center, P.C. - urologycenterpc.com
- Best Prostate Cancer Treatment Hospital In India - Medtripz - medtripz.com (2024)