
Prostate cancer treatment outcomes depend on measurable hospital quality signals — multidisciplinary coordination, radiation precision, surgical volume, and diagnostic infrastructure — not reputation alone.
This guide provides a five-step verification framework to evaluate prostate cancer hospitals using concrete operational metrics before admission.
Key Takeaways
- Verify weekly tumor board operations with documented treatment plans — co-location of specialists does not guarantee coordination
- Confirm AERB-certified radiation equipment (IGRT/IMRT) and reject hospitals relying on outdated cobalt-60 technology
- Target surgical centers performing ≥50 prostatectomies annually per surgeon for lower complication rates
- Check in-house pathology infrastructure to avoid 3-5 day diagnostic delays from outsourced labs
- Verify current CGHS empanelment status by phone before admission — online listings are often outdated
Why Choosing the Right Prostate Cancer Hospital Matters for Success Rates
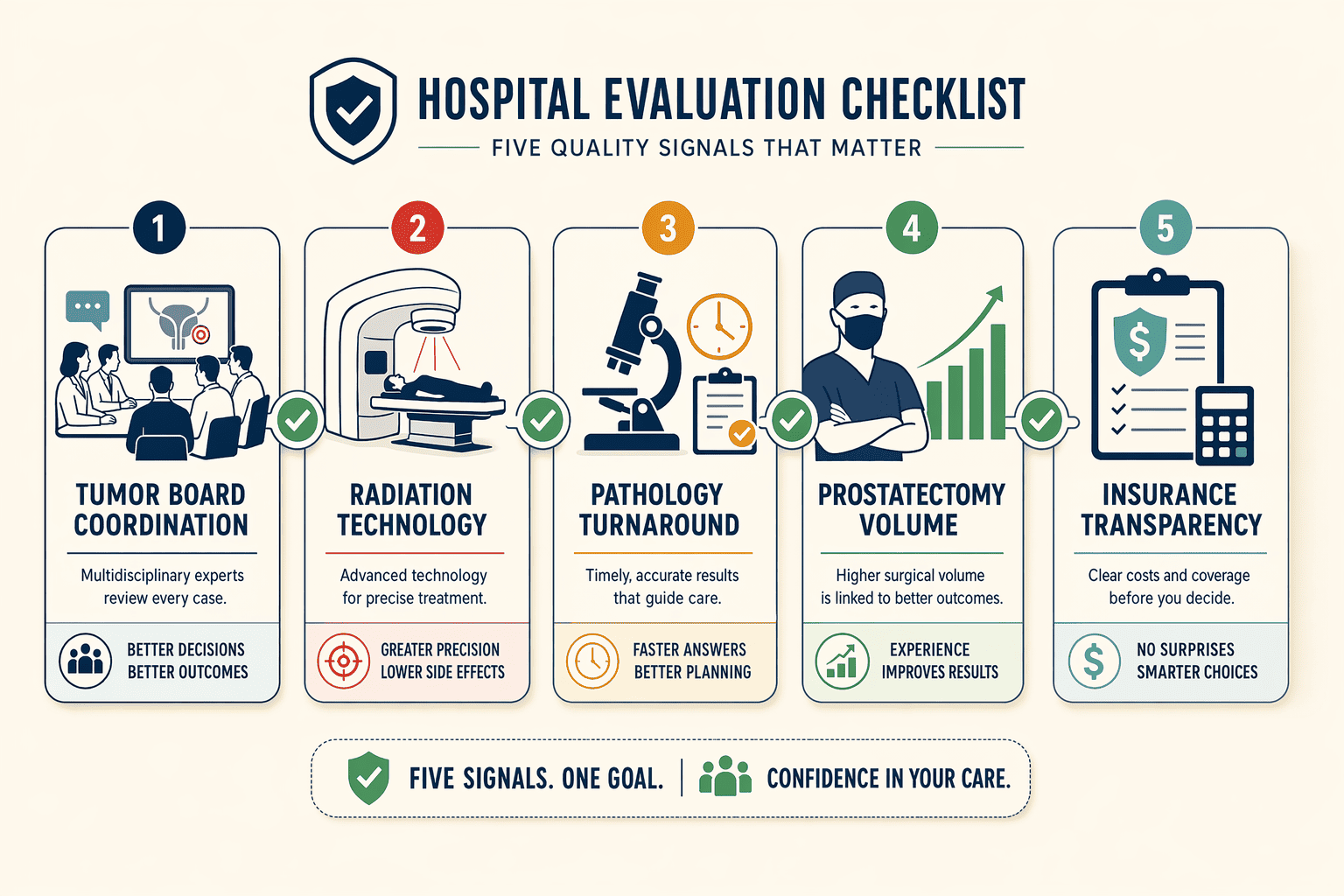
To choose a hospital for prostate cancer treatment with good success rates, verify five measurable quality signals: weekly tumor board operations (confirming multidisciplinary coordination actually occurs), radiation technology inventory (IGRT/IMRT/SBRT availability, not generic 'external beam'), diagnostic turnaround commitments (frozen-section timing, histopathology reporting windows), surgical case volume (prostatectomy numbers per year), and insurance empanelment transparency (oncology-specific coverage, not general-care empanelment only). These criteria matter because clinical stage, Gleason score, and PSA values together predict progression risk, and treatment decisions hinge on pathologic factors that require institutional capacity to assess rapidly.
The Complexity of Prostate Cancer Treatment
Stage-dependent pathways split localized prostate cancer (often managed with active surveillance, surgery, or radiation) from advanced disease requiring systemic therapy combinations. Multidisciplinary coordination becomes critical because prognostic variables—clinical TNM stage assessed through physical exam and biopsy, and pathologic staging requiring whole-gland evaluation, must inform a unified treatment plan. Hospitals may list both surgical and medical oncologists yet operate them in separate departments with minimal cross-consultation, leaving patients to coordinate handoffs themselves. Andromeda Cancer Hospital conducts weekly tumor board reviews where surgical, medical, and radiation oncologists review cases together, exemplifying the measurable coordination patients should verify elsewhere as well.
Why Traditional Hospital Rankings Fall Short
Listicle approaches, such as one naming five hospitals without methodology, skip the verification layer patients need. Conventional external beam radiation alone may lack the precision technology modern protocols require, yet rankings rarely confirm IGRT/IMRT inventory. Before admission, check: does the hospital publish tumor board frequency? Are frozen-section results available within 20-30 minutes, and is histopathology turnaround defined? Is oncology explicitly listed in insurance empanelment, or only general care? These process signals predict whether prognostic data will flow seamlessly across disciplines.
The first verification step separates hospitals with true multidisciplinary integration from those with co-located specialists working in silos.
Step 1: Verify Multidisciplinary Tumor Board Operations
What a Tumor Board Is and Why It Matters
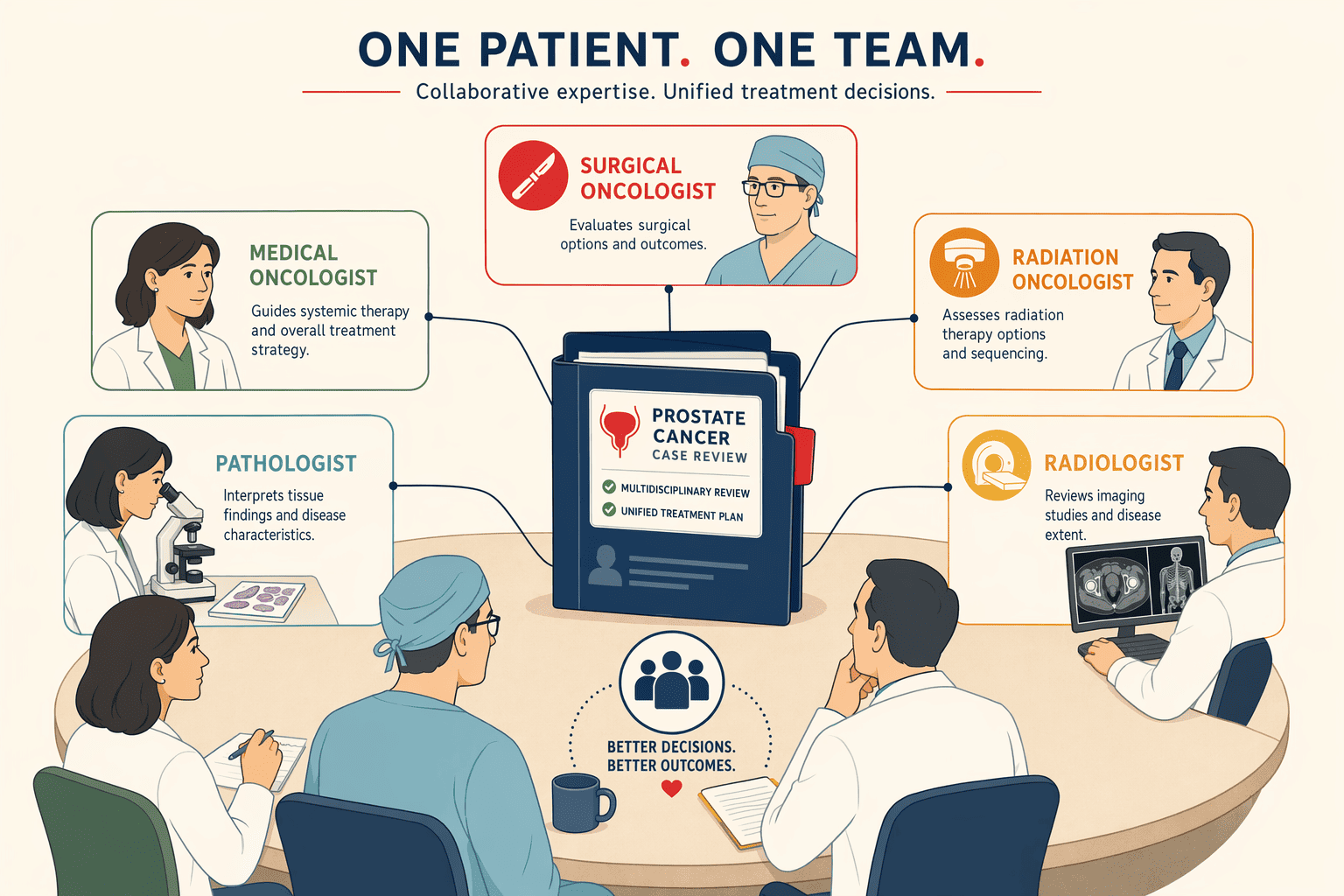
A multidisciplinary tumor board brings together surgical oncologists, medical oncologists, radiation oncologists, pathologists, and radiologists to review each patient's case and agree on a unified treatment plan. For prostate cancer, this coordination ensures that decisions about surgery, radiation, hormone therapy, or active surveillance reflect the combined expertise of specialists rather than a single doctor's perspective. Research shows that multidisciplinary clinics improve treatment adherence and reduce delays, outcomes that matter when prostate cancer biology varies widely from patient to patient.
The difference between having specialists under one roof and operating a functioning tumor board is documentation and meeting frequency. Physical proximity alone does not guarantee coordination, some hospitals list multiple oncologists yet operate them in separate departments with minimal cross-consultation.
How to Verify Board Frequency and Documentation
Ask these four questions when evaluating a hospital for prostate cancer treatment:
- How often does your tumor board meet, weekly, biweekly, or monthly?
- Are tumor board discussions documented with written treatment plans shared across specialties?
- Which specialists attend regularly, surgical oncology, medical oncology, radiation oncology, pathology, radiology?
- Can I request a copy of my tumor board discussion summary after my case is reviewed?
Hospitals with operational integration meet weekly or twice weekly and produce written summaries that all treating physicians can access. Andromeda Cancer Hospital, for instance, convenes multidisciplinary tumor board meetings twice weekly with surgical oncologists, oncoplastic breast surgeons, medical oncologists, radiation oncologists, radiologists, pathologists, and pain and palliative care specialists, one example among several hospitals that meet this standard. Quarterly meetings or verbal-only discussions signal weaker coordination, which can delay adjustments when prostate cancer progresses or when treatment side effects require multi-specialty input.
After confirming tumor board operations, the second step evaluates radiation technology generation and regulatory compliance.
Step 2: Check Radiation Technology Generation and AERB Licensing
Radiation precision directly affects side effects and cure rates. Verify the hospital's equipment generation and regulatory compliance before committing to treatment.
IGRT/IMRT Vs. Older Cobalt-60 Units
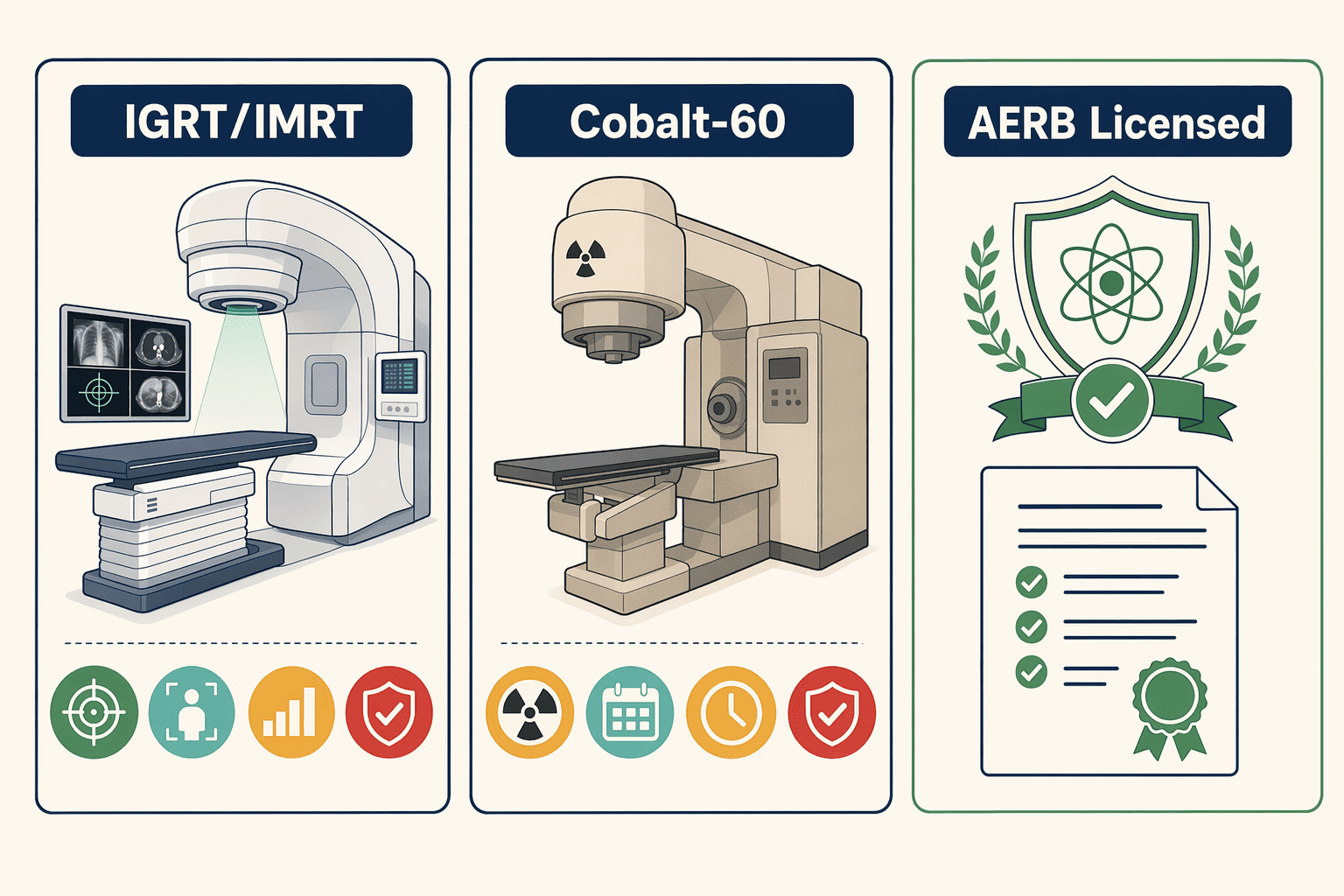
Modern radiation systems use image-guided radiotherapy (IGRT) and intensity-modulated radiotherapy (IMRT) to target tumors with millimeter precision while sparing healthy tissue. Older cobalt-60 machines deliver fixed-beam radiation without real-time imaging, functional for basic cases, but unable to adjust dose distribution based on daily organ position shifts. IMRT shapes radiation beams to match tumor contours; IGRT uses CT scans before each session to confirm target alignment. Listings on clinicspots.com and metrohospitals.com mention radiation therapy availability but do not explain whether the facility uses image-guided techniques or older technology, the precision gap patients must clarify before selecting a hospital. Ask: Does the radiation oncology department offer IGRT and IMRT? What machine model does the department use? Andromeda Cancer Hospital uses the Varian TrueBeam STx for image-guided radiotherapy, IMRT, VMAT, and stereotactic techniques, delivering global-standard precision radiation therapy.
How to Verify AERB Licensing
AERB (Atomic Energy Regulatory Board) certification is the legal requirement for operating radiation equipment in India. Hospitals without valid AERB licensing cannot legally perform PET-CT scans or radiation therapy, regulatory compliance is the minimum safety floor patients should verify. Check AERB licensing in three steps: Visit the AERB website and navigate to the public registry section. Search the hospital name in the certified institutions database. Confirm active certification status and verify the license covers radiation oncology and nuclear medicine departments. Andromeda Cancer Hospital operates an AERB-certified PET-CT facility, ensuring regulatory compliance across diagnostic and therapeutic radiation services. Hospitals that skip AERB certification or operate with expired licenses expose patients to unregulated radiation protocols, this verification step takes five minutes and confirms the institution meets national safety standards.
Radiation precision depends on diagnostic accuracy, the third step examines pathology and imaging infrastructure that feeds treatment planning.
Step 3: Evaluate Diagnostic Infrastructure and Turnaround Time
Why Turnaround Time Matters for Treatment Sequencing
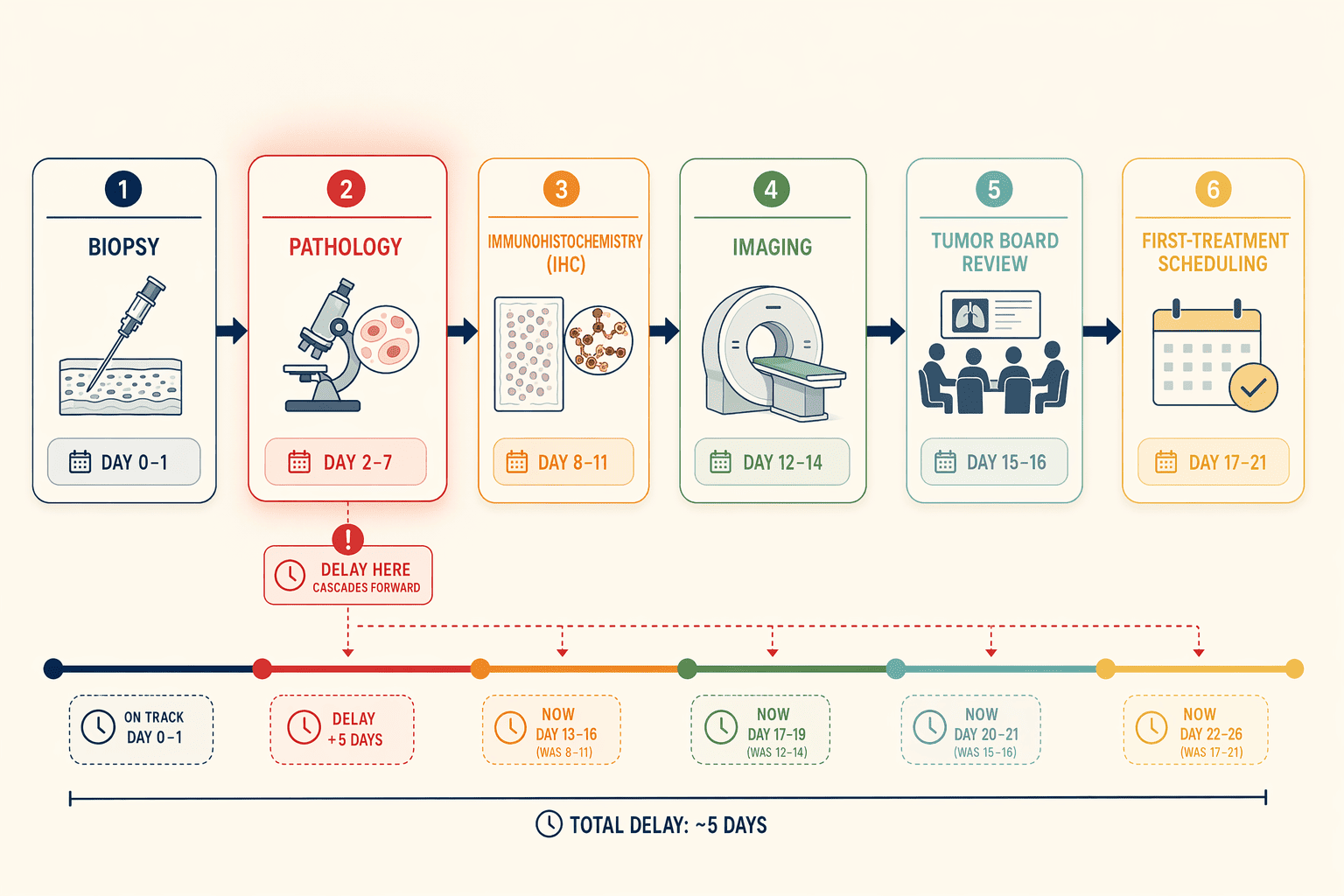
Diagnostic delays cascade into treatment delays, especially for time-sensitive advanced prostate cancer. Waiting two weeks for a biopsy report, then another week for immunohistochemistry results, then scheduling a tumor board review pushes first-treatment dates back by a month or more. For patients with aggressive disease or rising PSA, that month can shift staging and narrow treatment options. Before committing to a hospital, verify how quickly pathology, imaging, and molecular testing results reach your oncologist's desk.
In-House Vs. Outsourced Pathology Labs
Many hospital websites list diagnostic services without clarifying whether pathology runs in-house or through a partner lab. Some pages mention 'advanced diagnostic tools' and others describe 'thorough care under one roof' but omit turnaround-time specifics. Ask admissions teams directly: 'Is your pathology lab in-house or do you use a partner facility?' In-house labs typically deliver diagnostic histopathology within 48 to 72 hours. Outsourced arrangements can add 5 to 10 days. For PET-CT imaging, same-day or next-day reporting is critical for treatment planning timelines. Andromeda Cancer Hospital, for example, coordinates PET-CT plus IHC testing turnaround within one week for tumor board review, ensuring multidisciplinary treatment decisions aren't delayed by logistics. Molecular profiling for targeted therapies often takes longer, expect two to three weeks when accredited external labs handle genomic testing.
For patients considering surgery, the fourth step quantifies surgical expertise through case volume and complication reporting.
Step 4: Assess Surgical Volume and Outcomes Reporting
Why Surgical Volume Correlates With Outcomes
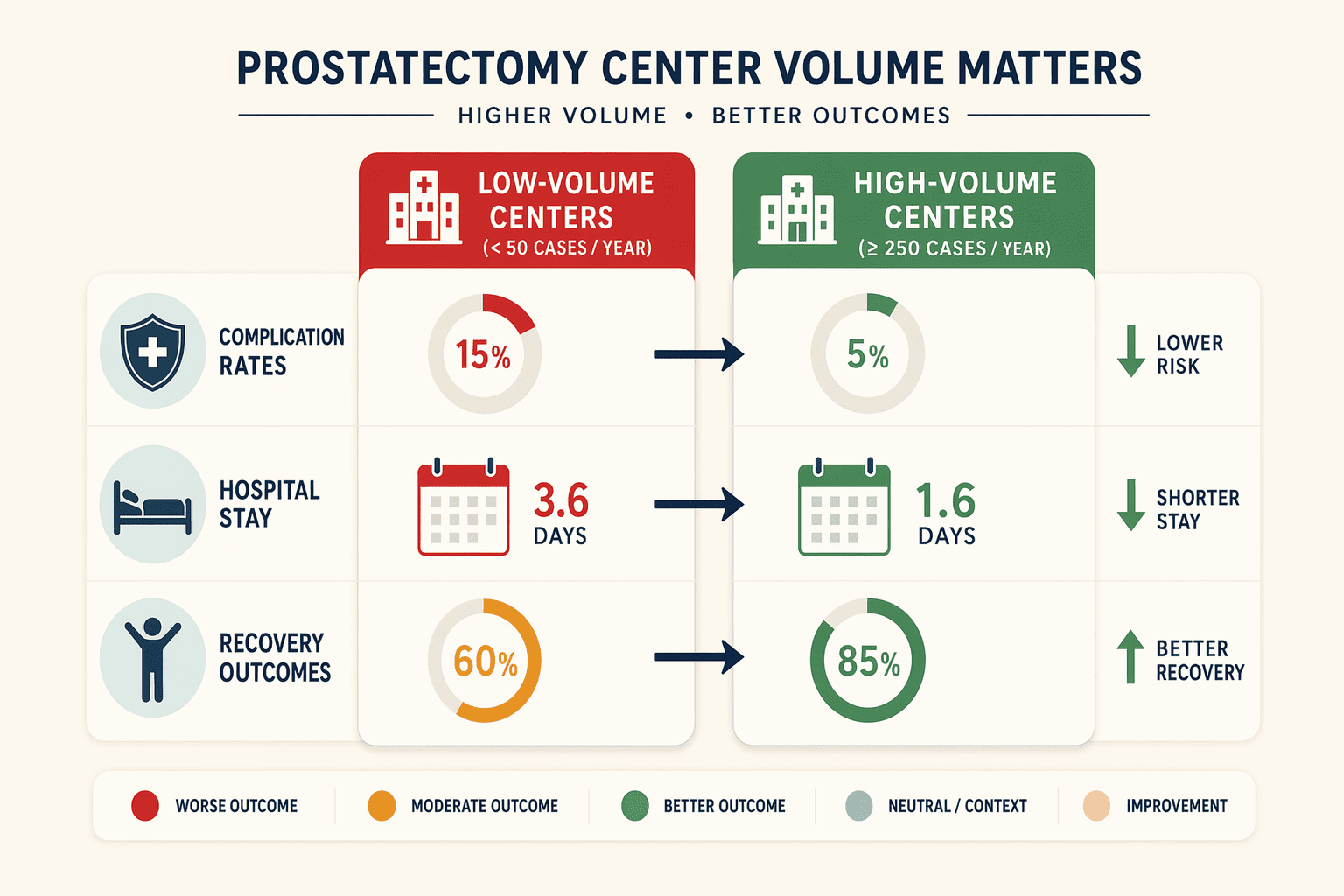
Academic research consistently demonstrates that higher prostatectomy case load correlates with better patient outcomes. Centers performing more than 50 radical prostatectomies annually report lower 90-day complication rates, shorter hospital stays, and improved functional recovery compared to low-volume facilities. This volume-outcome relationship reflects surgical team experience, refined protocols, and infrastructure investment that only high case loads sustain. Centralization of prostate cancer care into specialized hubs has been implemented across Europe and parts of the United States to concentrate expertise. The hub-and-spoke model directs complex cases to high-volume centers while maintaining local access for routine follow-up. Specialized prostate cancer programs, not general oncology departments, tend to achieve the case volumes that drive measurability and quality improvement.
How to Ask About Case Load and Complication Rates
When evaluating a hospital's surgical program, ask three verification questions: (1) How many prostatectomies does your team perform annually? Target centers reporting ≥50 cases per surgeon. (2) What is your 90-day complication rate for radical prostatectomy? Request stratified data by stage and approach (open, laparoscopic, robotic). (3) Do you participate in national outcomes registries or publish audit data? Registry participation signals transparency and external benchmarking. Thorough prostate cancer clinics like The Urology Center of Colorado's specialized program model this approach, publishing volume and outcomes data publicly. Andromeda Cancer Hospital's urological oncology program represents another example of specialized care concentration. Remember: not every prostate cancer patient requires surgery, treatment sequencing depends on stage and tumor biology. Volume matters when surgery is indicated, but volume alone does not determine whether surgery is the right choice for your case.
The fifth step addresses financial transparency and insurance coverage, practical constraints that determine treatment access regardless of clinical quality.
Step 5: Confirm Insurance Empanelment and Cost Transparency
CGHS and ECHS Empanelment Verification
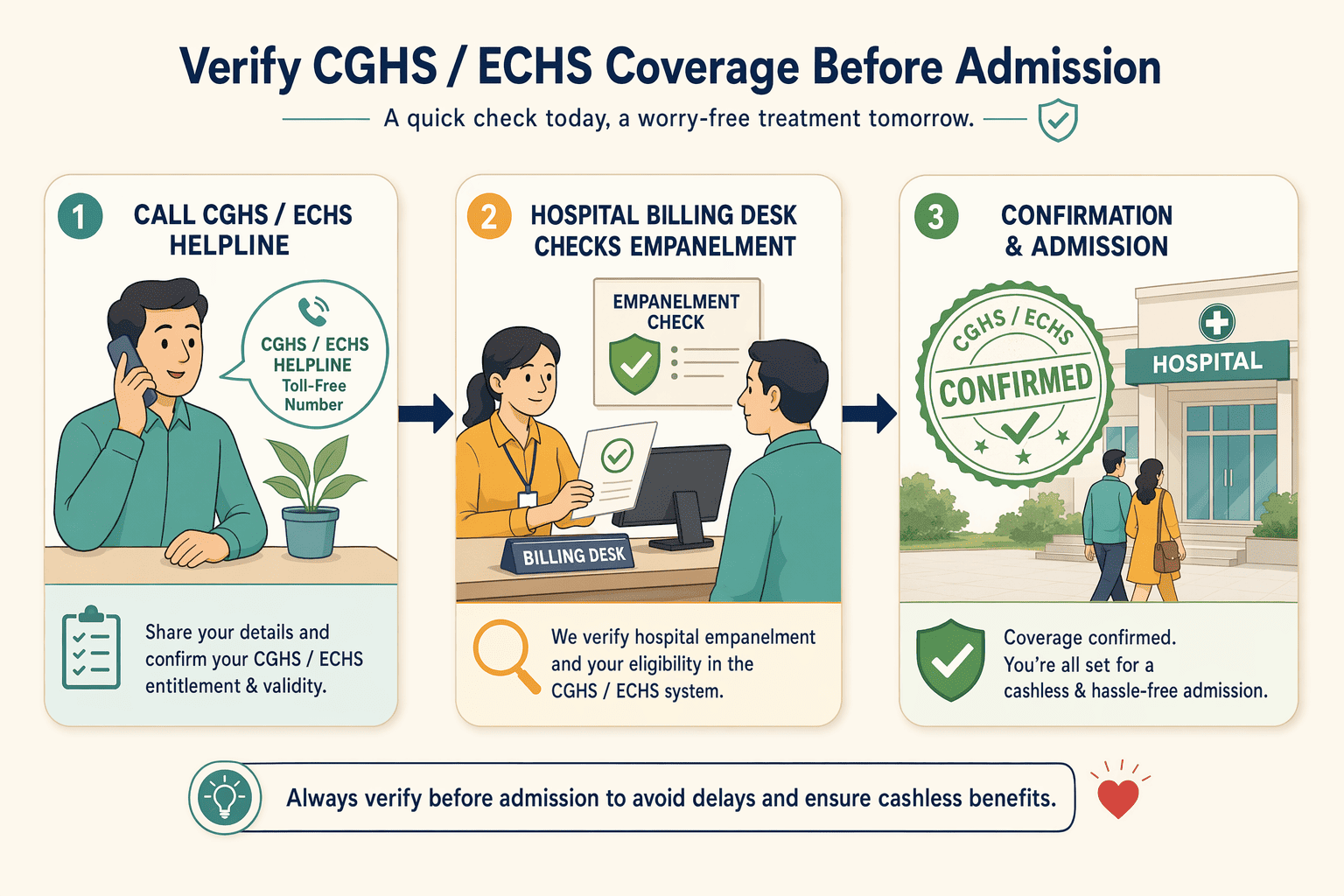
CGHS empanelment status changes periodically and must be verified before admission, not assumed from outdated online listings. Call the CGHS helpline or the hospital's billing desk to confirm current empanelment before you schedule surgery or radiation planning. Hospitals that participate in CGHS frameworks, such as CGHS cancer treatment facilities, simplify documentation and coordinate with CGHS offices to ensure beneficiaries receive covered services. Asking for a written confirmation of empanelment and the covered procedures prevents billing surprises after treatment starts.
Cost Transparency for Multimodal Treatment
Private-cost variation depends on treatment modality combination, surgery plus radiation differs from radiation-only in sequencing, anesthesia, and inpatient stay. Request itemized estimates broken down by modality, not single aggregate ranges that obscure each phase's cost. Clinics that provide upfront, detailed cost structures, like the Thorough Prostate Cancer Clinic model, set a best practice: patients see tracer type, scan protocol, and professional fees line by line. Ask your hospital's financial counselor for a written breakdown before signing consent forms, transparency at the estimate stage protects you from unexplained charges during or after multimodal care.
The five-step framework translates into concrete operational differences when applied to Delhi NCR hospitals.
Applying the Framework: Institutional Examples in Delhi NCR
How Leading Centers Measure up on the 5 Criteria
The five-step verification framework, multidisciplinary coordination, radiation precision, surgical expertise, diagnostic turnaround, and insurance coverage, translates into concrete operational differences across Delhi NCR hospitals. The table below shows how four institutions score on key indicators:
| Criterion | Andromeda Cancer Hospital | Medanta – The Medicity | Apollo Hospitals | Fortis Memorial Research Institute |
|---|---|---|---|---|
| Tumor Board Frequency | Twice weekly | Weekly | Weekly | Weekly |
| Radiation Technology | IGRT, IMRT, VMAT, SBRT | IGRT, IMRT available | IGRT, IMRT available | IGRT, IMRT available |
| Robotic Prostatectomy | Certified Da Vinci surgeon on staff | Available | Available | Available |
| Accreditation | NABL-trained pathology team | NABH, JCI | NABH, JCI | NABH, JCI |
This comparison illustrates the framework in action: Andromeda Cancer Hospital operates twice-weekly tumor boards and offers advanced radiation techniques including stereotactic body radiotherapy, while the other three centers maintain weekly boards and comparable IGRT/IMRT capabilities. All four provide robotic prostatectomy, meeting the surgical volume and technology criterion, and maintain quality-system oversight through accreditation or specialized training.
Choosing the Right Fit for Your Case
Not every patient needs all five signals equally. A man with localized, low-risk prostate cancer (PSA <10, Gleason 6) may prioritize surgical volume and radiation precision, ensuring the hospital performs high-volume prostatectomies and offers image-guided boost techniques. A patient with metastatic disease, in contrast, should weight multidisciplinary coordination and insurance empanelment more heavily: systemic therapy sequences depend on tumor biology, and treatment costs escalate when hormone therapy, chemotherapy, or novel agents enter the plan.
The institutional examples above show that multiple Delhi NCR centers meet the framework's core criteria. Andromeda Cancer Hospital provides personalized treatment through twice-weekly multidisciplinary discussions guided by international guidelines, one model of operational integration. Medanta, Apollo, and Fortis offer weekly boards and comparable technology suites. The choice hinges on which criteria matter most for your stage, biology, and logistics: proximity, insurance network alignment, and the specific sub-specialists involved in your case.
Conclusion
High-volume centers with specialized prostate cancer programs offer better surgical outcomes but may have longer wait times for first appointments compared to smaller general oncology centers, prioritize volume when surgery is indicated. Hospitals with in-house pathology labs deliver faster diagnostic turnaround but may have higher upfront costs compared to centers that outsource to partner facilities, weigh speed against budget constraints for your case.
As precision oncology advances, prostate cancer treatment will increasingly rely on molecular profiling and AI-assisted imaging to personalize therapy, choosing hospitals with modern diagnostic infrastructure and documented multidisciplinary coordination positions patients to benefit from these innovations.
Apply the 5-step framework to evaluate Andromeda Cancer Hospital's multidisciplinary prostate cancer program, verify our tumor board operations, AERB-certified radiation technology, and surgical volume before your first consultation.
Frequently Asked Questions
Does my hospital need AERB certification for prostate cancer treatment?
Yes, AERB certification is legally required for operating radiation equipment and PET-CT scanners in India. Hospitals without valid AERB licensing cannot legally perform radiation therapy or nuclear imaging. Verify AERB status before admission to ensure regulatory compliance and equipment safety standards.
How do I verify tumor board activity at a hospital?
Ask four verification questions: (1) How often does your tumor board meet? (2) Are meetings documented? (3) Which specialists attend? (4) Can I request a copy of my discussion summary? These questions distinguish operational integration from simple co-location of specialists under one roof.
What is the difference between IGRT/IMRT and cobalt-60 radiation?
IGRT/IMRT uses image-guided, intensity-modulated systems that target tumors with millimeter precision while sparing healthy tissue. Cobalt-60 machines deliver fixed-beam radiation without real-time imaging adjustment. Hospitals with older cobalt-60 units cannot deliver IGRT or IMRT precision, technology generation directly affects side effects.
Does higher surgical volume always mean better prostate cancer outcomes?
Academic research shows higher prostatectomy case load correlates with lower 90-day complication rates and shorter hospital stays. However, not every patient requires surgery, treatment depends on cancer stage and biology. Surgical volume matters only when surgery is clinically indicated for your case.
How do I check if a hospital is empanelled under CGHS?
Call the CGHS helpline or the hospital's billing desk to confirm current empanelment status before scheduling treatment. CGHS empanelment status changes periodically and must be verified before admission, do not rely on outdated online listings that may show expired empanelment.
Can I request a copy of my tumor board discussion?
Yes, patients have the right to request documentation of their multidisciplinary tumor board discussion. Written treatment plans demonstrate operational integration. Hospitals with functioning tumor boards produce documented summaries accessible to all treating physicians, ensuring coordinated care across specialties.
What if my hospital outsources pathology — does that delay treatment?
Outsourced pathology labs typically add 3-5 business days compared to in-house facilities. Turnaround time for diagnostic reports varies by in-house versus outsourced pathology infrastructure. Ask upfront whether the hospital runs pathology in-house or partners with external labs to estimate diagnostic timeline.