
Hospital websites promise thorough cancer care, but marketing claims rarely reflect operational reality. Patients need verification tools to audit multidisciplinary coordination, diagnostic depth, and survivorship programs before admission.
Key Takeaways
- Thorough cancer care requires weekly tumor boards, AERB-certified equipment, same-roof oncology departments, in-house pathology with IHC, and structured survivorship programs
- Marketing department listings do not prove operational integration — verify tumor board meeting schedules, pathology turnaround times, and care coordination protocols
- AERB certification confirms radiation and nuclear medicine equipment meet Indian safety standards; hospitals without it may use outdated or unsafe technology
- CGHS empanelment covers diagnosis through follow-up at 27 recognized cancer hospitals, but patients must verify which specific services are included
- Survivorship care extends beyond routine appointments to include late-effects monitoring, rehabilitation referrals, and documented care transition plans
What 'All Treatment Stages' Actually Means in Cancer Care
When evaluating which cancer hospitals provide all treatment stages from diagnosis to follow-up care, verify five operational signals: twice-weekly tumor boards with documented minutes, surgical, medical, and radiation oncology co-located within the same facility, in-house pathology with frozen-section capability, AERB-certified radiation equipment, and survivorship clinic protocols for long-term follow-up. Marketing brochures listing departments do not prove coordination — ask for tumor board frequency and care-pathway documentation before assuming integration.
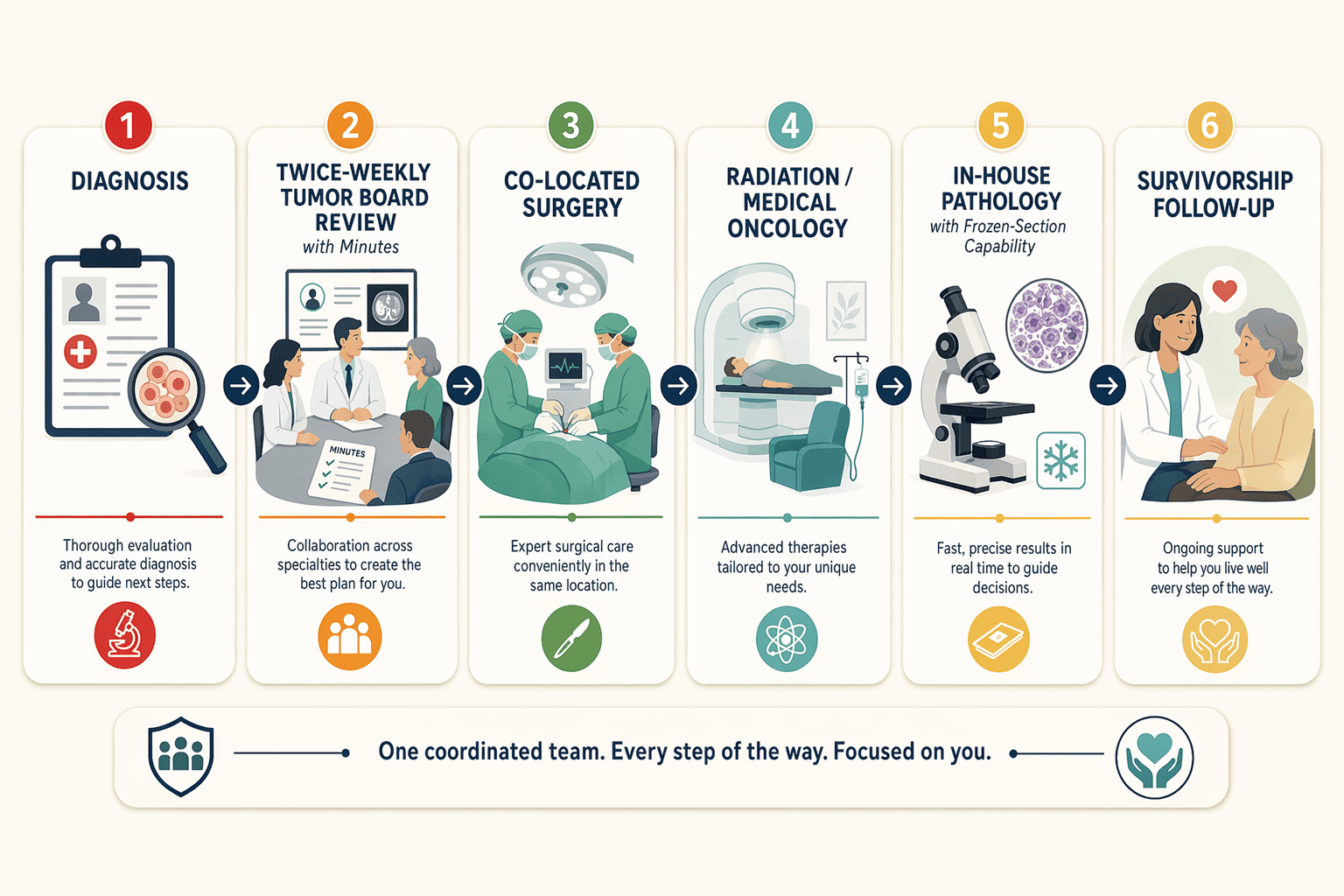
The Five Core Treatment Stages
Thorough cancer care spans five operational stages: diagnosis (imaging, biopsy, pathology reporting within 7–10 days), treatment planning (multidisciplinary tumor board review with surgical, medical, and radiation oncologists ), active treatment (surgery, chemotherapy, radiation administered according to board-approved protocols), transitional care (post-treatment symptom management, wound care, nutritional support), and long-term follow-up (survivorship clinic visits, late-effect monitoring, recurrence surveillance imaging). Not every patient requires every treatment modality — sequencing depends on cancer type, stage, and biology. Andromeda Cancer Hospital operates as a 105-bed tertiary oncology facility with twice-weekly tumor boards and same-roof medical, surgical, and radiation oncology.
Why 'Under One Roof' Differs From 'Operational Integration'
Physical co-location of oncology departments does not guarantee coordinated care — some hospitals maintain separate surgical and medical oncology divisions with minimal cross-consultation. Integration requires shared electronic health records, documented tumor board participation, and written care transitions between stages. Verify tumor board meeting frequency (weekly minimum), pathology turnaround times for immunohistochemistry (IHC), and whether radiation oncologists review surgical margins before planning treatment fields. Hospitals that merely list departments without showing coordination mechanisms often defer complex cases to tertiary centers mid-treatment.
Book An Appointment at Andromeda Cancer Hospital to review your case in our twice-weekly multidisciplinary tumor board.
Thorough care claims appear in every hospital brochure, but operational verification requires specific audit questions that distinguish coordinated oncology teams from fragmented department silos.
How to Verify Multidisciplinary Coordination (Not Just Department Listings)
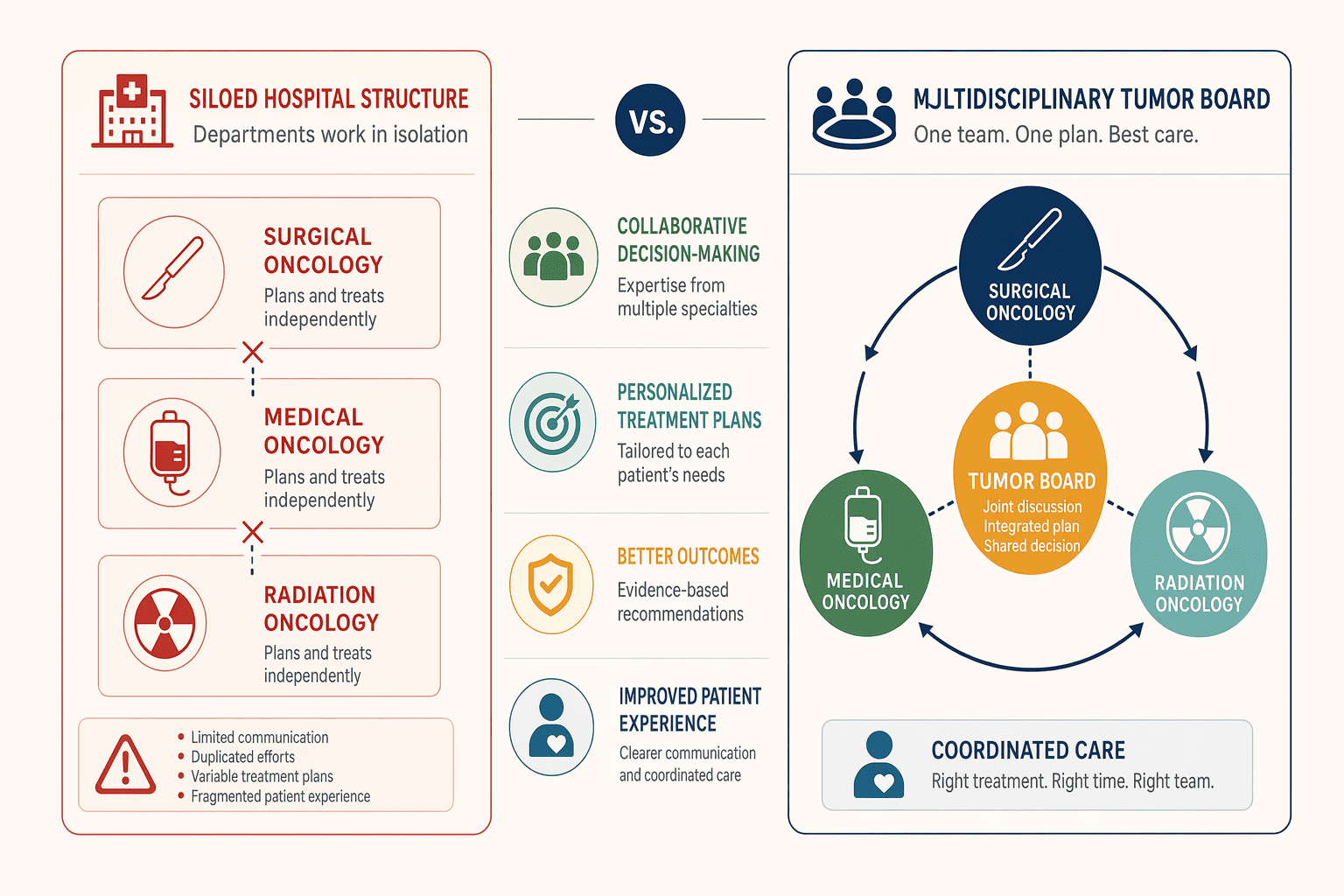
Marketing materials listing oncology departments do not prove weekly tumor board activity. Hospitals such as Max Healthcare and Apollo Cancer Centers mention "multidisciplinary care" without documenting the frequency of tumor board meetings or the participation of all required specialists. To evaluate whether a hospital genuinely coordinates treatment across surgical, medical, and radiation oncology — rather than operating specialty departments in silos, readers must ask for specific documentation of tumor board processes.
Weekly Tumor Board Documentation and Access
A tumor board is a scheduled meeting in which surgical oncologists, medical oncologists, radiation oncologists, radiologists, and pathologists review each newly diagnosed cancer case to develop a coordinated treatment plan. Active oncology centers typically convene tumor boards weekly; high-volume institutions may meet twice weekly. Patients should verify that the hospital documents tumor board decisions and provides meeting summaries or case-review notes upon request. Andromeda Cancer Hospital, for example, convenes multidisciplinary tumor board meetings twice weekly to ensure coordinated treatment planning across specialties, and patients receive written summaries of the recommendations. Without documented tumor board activity, specialists may recommend treatment independently, leading to inconsistent or duplicated interventions.
Multidisciplinary Team Composition: Who Should Be Present
An effective tumor board includes core representatives from surgical oncology, medical oncology, radiation oncology, diagnostic radiology (including interventional radiology when relevant), pathology, and pain and palliative care. At Andromeda Cancer Hospital, the tumor board brings together surgical oncologists, oncoplastic breast surgeons, medical oncologists, radiation oncologists, radiologists, pathologists, and pain and palliative care specialists. Patients should confirm that all these disciplines attend regularly, not just on paper, by asking to review sample meeting rosters or agendas. A tumor board listing only surgical and medical oncologists without radiology or pathology representation does not meet evidence-based standards for multidisciplinary care.
Questions to Ask About Care-Pathway Documentation
To verify that tumor board recommendations are communicated to patients, not only circulated internally, readers should ask the following questions:
- How often does the tumor board meet?
- Can I review a sample case summary or meeting minutes?
- Which specialists attend each tumor board meeting?
- Will I receive a written summary of the tumor board's treatment recommendation for my case?
- How are tumor board decisions communicated to the treating physicians and to me?
Hospitals that cannot answer these questions may list multidisciplinary departments without implementing multidisciplinary care pathways, leaving patients to navigate fragmented treatment decisions across multiple specialties.
Tumor board coordination depends on diagnostic infrastructure that can deliver accurate results within treatment planning windows, making equipment certification and pathology integration the foundation of multidisciplinary care.
On-Site Diagnostic Depth: AERB Certification and Pathology Integration
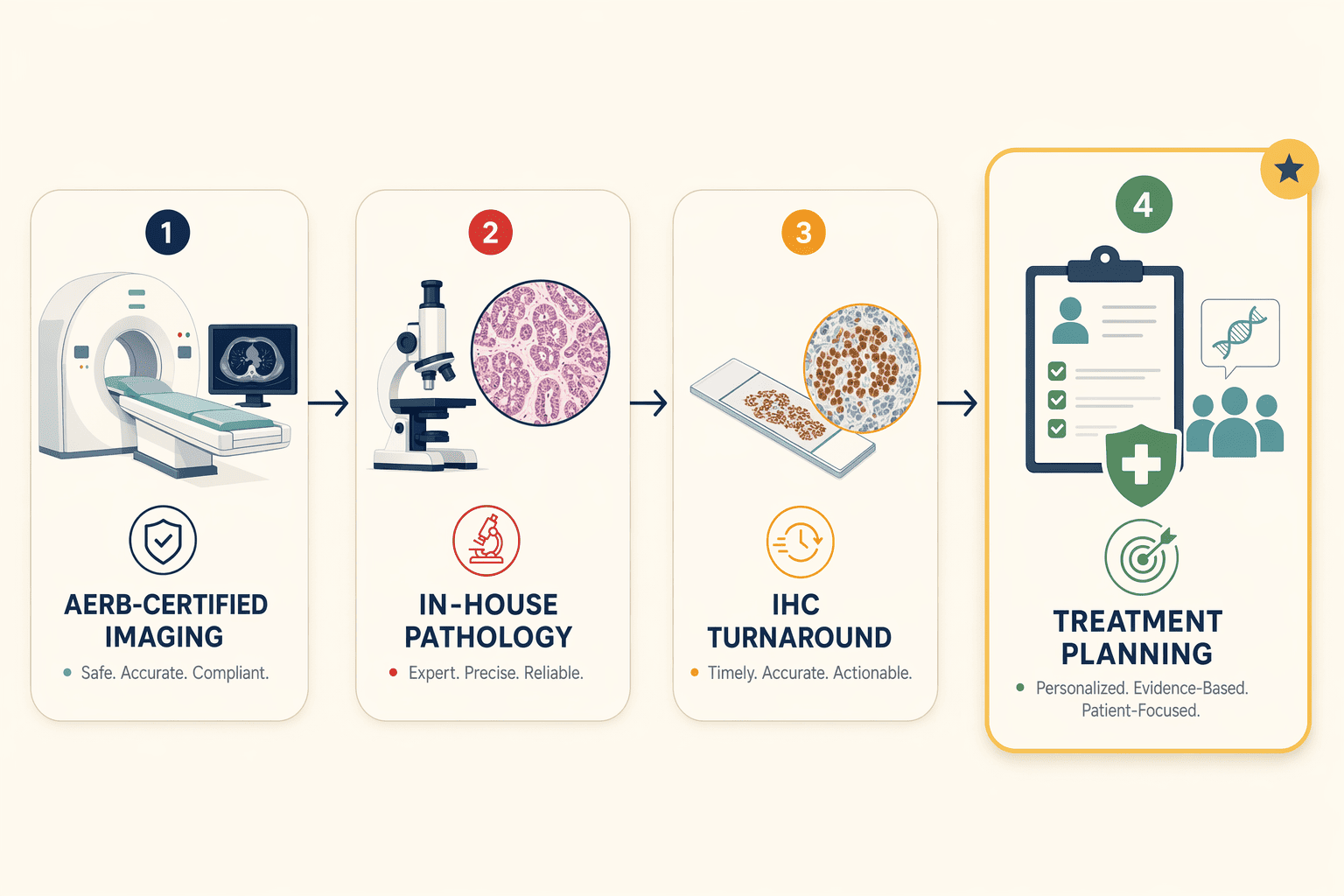
Hospital directories list dozens of cancer facilities by name, Singhla Medicos and Vaidam enumerate providers across northern India, but rarely surface the regulatory and operational signals that distinguish integrated diagnostics from outsourced services. Three verification checkpoints expose diagnostic depth: AERB certification for imaging and radiation equipment, in-house pathology capability, and immunohistochemistry (IHC) turnaround times. Patients who audit these signals before admission secure faster treatment planning and reduce the risk of coordination delays that fragment care.
AERB Certification Lookup Process
The Atomic Energy Regulatory Board (AERB) certifies hospitals to operate PET-CT scanners, radiation therapy equipment, and nuclear medicine facilities under India's radiation safety framework. Certification confirms that equipment meets safety standards, staff hold appropriate licenses, and the facility maintains radiation protection protocols. To verify a hospital's AERB status, request the facility's radiation safety officer (RSO) certificate and cross-reference the hospital name against the AERB public registry, hospitals lacking active certification operate imaging or radiation equipment without regulatory oversight. Andromeda Cancer Hospital operates an AERB-certified PET-CT facility equipped with the GE Discovery IQ 2 system, meeting the baseline requirement for nuclear medicine in oncology diagnosis and therapy planning.
In-House Pathology Vs. Outsourced Diagnostics
Hospitals with on-site pathology labs process tissue samples, conduct frozen section analysis during surgery, and deliver histopathology reports within days, eliminating the courier delays and communication gaps inherent in outsourced diagnostics. Facilities that send biopsies to external reference labs introduce 3-7 day turnaround extensions and rely on email or phone to relay results, fragmenting the care team's ability to convene same-week tumor board discussions. Andromeda Cancer Hospital coordinates PET-CT, MRI, and IHC testing under one roof, enabling same-week multidisciplinary tumor board review. Patients should confirm whether the hospital's pathologist attends tumor board meetings in person, outsourced pathology arrangements rarely include direct pathologist participation, weakening the diagnostic foundation for treatment planning.
IHC Turnaround Time and Outsourcing Partnerships
Immunohistochemistry (IHC) testing identifies tumor protein markers that guide targeted therapy selection, HER2 status in breast cancer, PD-L1 expression in lung cancer, MSI-H markers in colorectal cancer. Hospitals that perform IHC in-house typically return results within 3-5 business days; those outsourcing IHC to accredited reference labs face 7-14 day delays, postponing chemotherapy initiation or surgical scheduling. Ask three questions before admission: (1) Does the hospital perform IHC testing on-site or through a partner lab? (2) What is the documented turnaround time from biopsy to IHC report availability? (3) Are IHC results integrated into the hospital's electronic health record, or delivered as standalone PDFs requiring manual review? Andromeda Cancer Hospital has coordinated PET-CT (https://www.andromedahospital.in/treatments/nuclear-medicine-pet-ct) and IHC testing, with a turnaround within one week for tumor board review, meeting the operational threshold for treatment decisions without diagnostic bottlenecks.
The 3-step decision framework: (1) Verify AERB certification for radiation and nuclear medicine equipment by requesting the RSO certificate and checking the public registry. (2) Ask whether pathology, including IHC, is performed in-house and confirm the documented turnaround time from biopsy to report. (3) Confirm whether imaging and pathology reports are integrated into the hospital's electronic health record or delivered as separate documents requiring manual coordination. Hospitals that satisfy all three criteria eliminate the diagnostic fragmentation that delays multimodal treatment planning and prolongs time-to-first-dose for chemotherapy or radiation.
Diagnostic depth matters only when treatment delivery capabilities exist under one roof, eliminating the care fragmentation that occurs when patients shuttle between separate facilities for surgery, chemotherapy, and radiation.
Treatment Delivery Capabilities: Surgery, Radiation, Systemic Therapy Under One Roof
Same-Roof Vs. Same-Network: Why It Matters
Physical co-location differs fundamentally from operational integration. Some multi-hospital networks claim thorough cancer care but require patients to travel between facilities for surgical oncology, systemic therapy, and radiation therapy. Metro Hospitals' CGHS chemotherapy services, for instance, offer advanced systemic therapy without same-roof surgical or radiation oncology, patients must coordinate across separate locations for complete treatment.
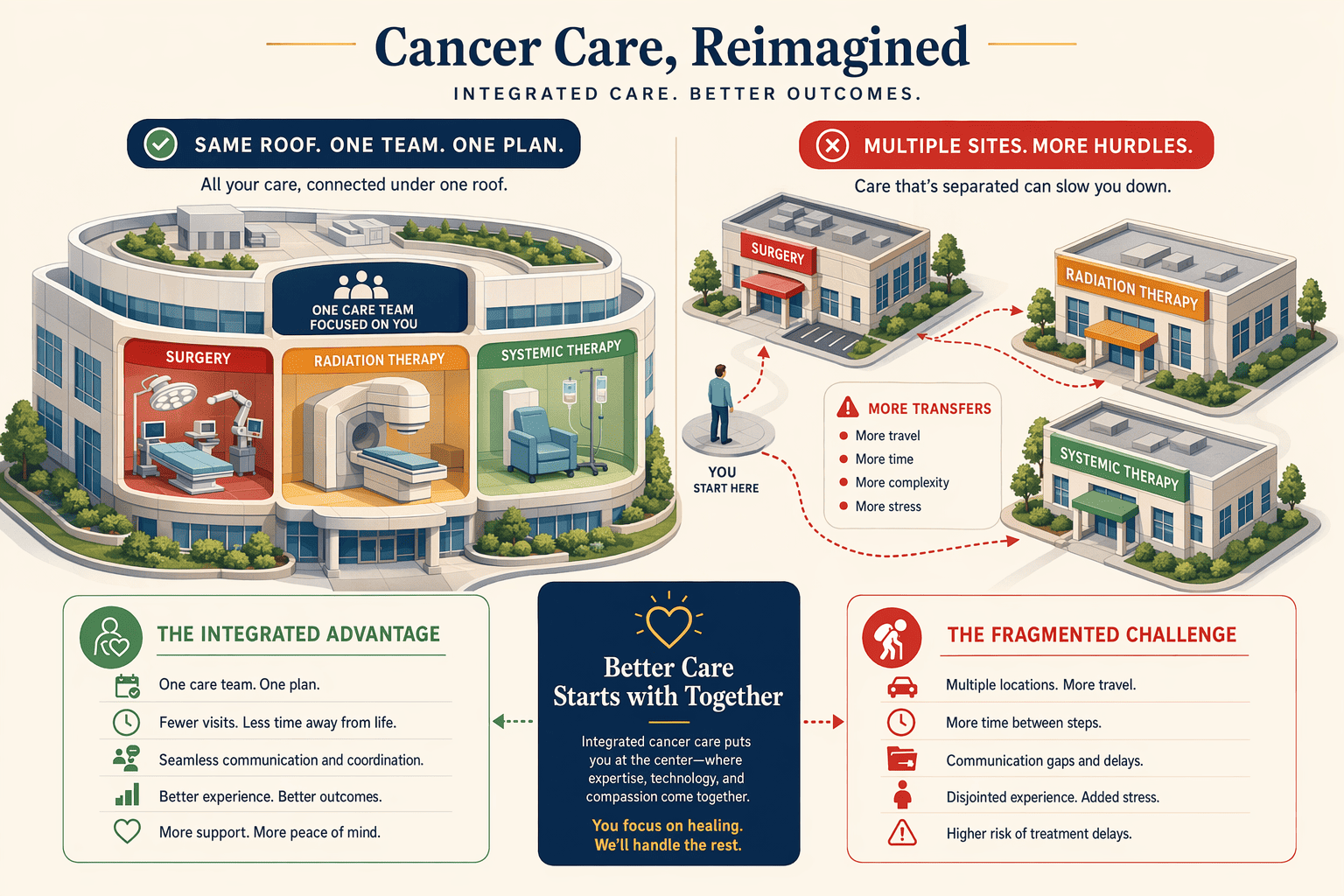
Andromeda Cancer Hospital offers surgical oncology, medical oncology, and radiation oncology under one roof, enabling joint tumor board review, shared care plans, and integrated scheduling. NYC Health + Hospitals' Metropolitan Cancer Center illustrates the international benchmark: multidisciplinary teams support patients from prevention through survivorship in a single facility, eliminating the coordination burden of multi-site care.
Brachytherapy, Safe Chemotherapy Prep, and Daycare Beds
Less than 50% of tertiary hospitals in India offer key services like brachytherapy, safe chemotherapy preparation, or daycare beds; only 41.6% of public tertiary hospitals have dedicated paediatric oncology departments. These capabilities signal operational depth beyond basic modality availability. Brachytherapy, delivering radiation internally, requires specialized licensing and physics support. Safe chemotherapy preparation demands pharmacy infrastructure compliant with handling cytotoxic agents. Daycare infusion beds allow outpatient systemic therapy, reducing hospitalization costs and infection risk.
Andromeda Cancer Hospital provides a fully equipped chemo-daycare facility and integrated radiation oncology capabilities, ensuring that patients access the full spectrum of treatment modalities without referral to external centers.
Questions to Ask About Modality Integration
To verify operational integration beyond physical co-location, patients should ask:
- Does the hospital hold weekly tumor boards where surgical, medical, and radiation oncologists review cases together?
- Are follow-up appointments scheduled with the entire care team at once, or must I coordinate separate visits?
- If I need chemotherapy before surgery, will my oncologist and surgeon communicate directly, or through paper referrals?
- Does the facility offer brachytherapy, safe chemotherapy preparation under a laminar-flow hood, and daycare infusion beds on-site?
These questions distinguish marketing claims from care coordination. Same-building specialists don't guarantee shared care plans, verify that the hospital's operational model supports integrated treatment delivery across all modalities.
Treatment delivery represents the acute phase of cancer care, but thorough hospitals extend coordination into the survivorship phase with structured follow-up protocols that most facilities describe vaguely as 'continued support.'
Survivorship and Follow-Up Programs: What to Ask Beyond 'We Offer Follow-Up'
When hospitals claim they provide 'complete care from diagnosis to follow-up,' most patients assume that means structured survivorship programs. It doesn't. Generic follow-up appointments, often just imaging reviews and symptom checks, lack the late-effects monitoring, rehabilitation planning, and care transition documentation that define evidence-based survivorship care. Without asking specific questions before admission, you may discover months after treatment that what was promised as thorough follow-up is actually reactive check-ins with no protocol for long-term surveillance or quality-of-life support.
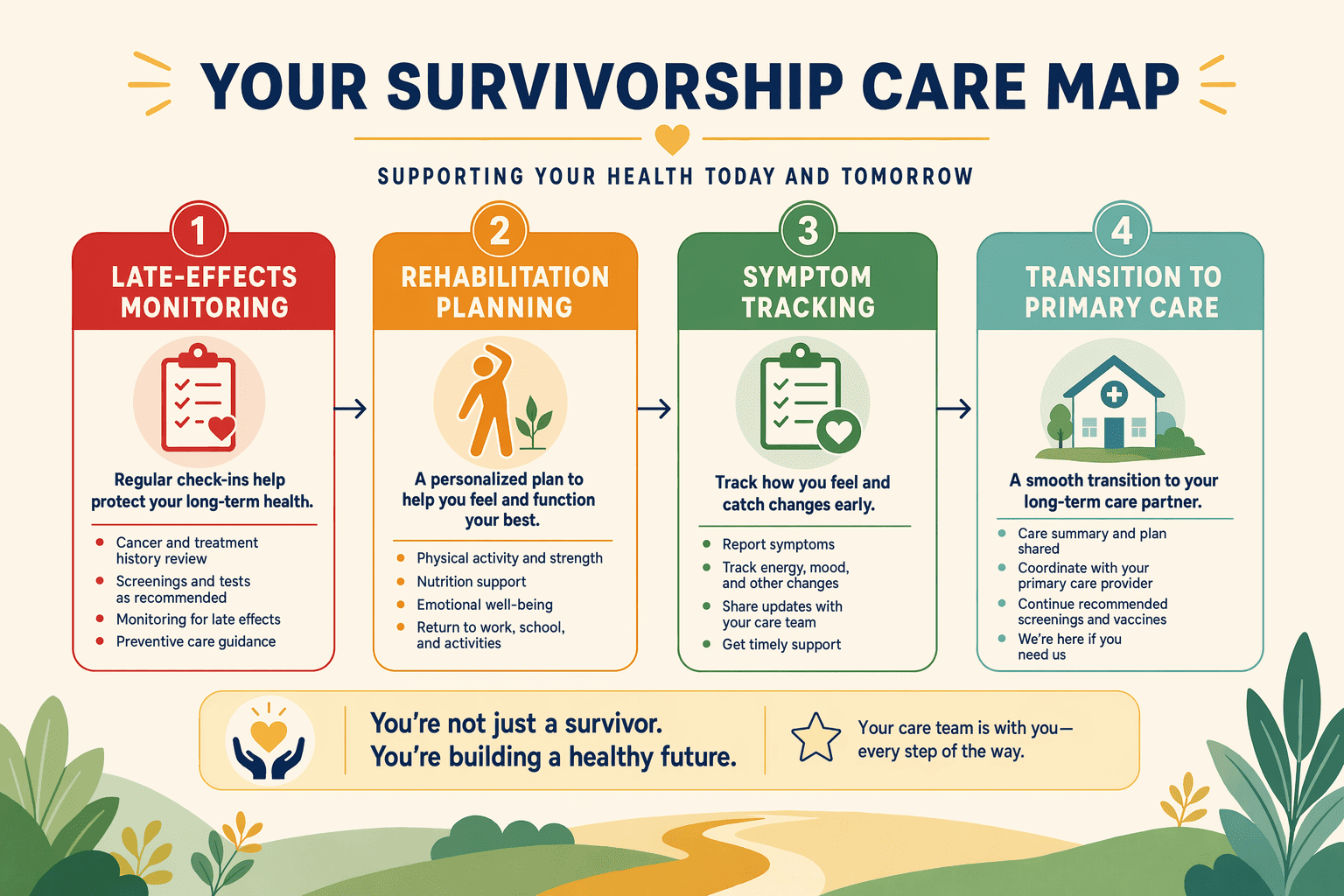
What Survivorship Care Programs Include
Structured survivorship care extends far beyond routine follow-up visits. Evidence-based programs integrate late-effects monitoring (tracking cardiovascular, bone health, and endocrine complications from treatment), rehabilitation services (physical therapy for lymphedema, speech therapy after head and neck surgery), psychosocial support (counseling for anxiety, depression, and survivorship adjustment), and care transition planning that documents your treatment summary and hands you off to primary care with clear surveillance protocols. Ask: Is there a dedicated survivorship clinic or coordinator? What surveillance imaging schedules do you follow? Do you provide rehabilitation referrals and psychosocial support?
Long-Term Follow-Up Protocols and Documentation
Long-term follow-up protocols, not ad hoc appointments, define how proactively a hospital monitors you after primary treatment ends. Verify that the hospital follows published surveillance guidelines for your cancer type: imaging schedules (PET-CT, MRI, or mammography at specified intervals), biomarker monitoring (tumor markers, hormone levels), and recurrence risk assessment updated as new data emerge. Documentation matters: your treatment summary should list every chemotherapy cycle, radiation dose, surgical procedure, and known late effects so your primary care physician or a future oncologist can interpret new symptoms correctly. Ask: Do you document care transition plans? How do you communicate my treatment history to my primary care team?
Patient Navigation and Support Services During Treatment Transitions
Patient navigators coordinate the handoff from active treatment to survivorship by scheduling follow-up appointments, arranging rehabilitation referrals, connecting you to support groups, and verifying that your insurance covers long-term services. Cancer treatment can be very expensive, and navigators help you understand which follow-up imaging and rehabilitation visits your plan covers under CGHS or private insurance. Hospitals that claim complete care but assign no navigator leave you to decode insurance codes and appointment logistics alone. Ask before admission: Is there a patient navigator assigned to my case? What support services are included during care transitions?
The anti-pattern: assuming that a hospital offering 'follow-up care' has structured survivorship protocols. Without documented surveillance schedules, late-effects monitoring, and care transition plans, follow-up becomes reactive, you report symptoms, the team responds, rather than proactive surveillance that catches complications early. Ask for the survivorship clinic's protocols in writing before choosing your hospital.
The preceding sections identified operational signals that define thorough cancer care, this final section consolidates those signals into a step-by-step verification checklist for prospective patients.
Evaluating Thorough Cancer Hospitals: a Step-By-Step Checklist
Pre-Admission Verification Checklist
Ask these questions before admission to verify a hospital's thorough-care claims are operational, not marketing:
- Tumor board frequency: Does the hospital convene multidisciplinary tumor boards at least weekly, with documented participation by surgical, medical, and radiation oncologists plus pathologists? At Andromeda Cancer Hospital, tumor board meetings occur twice weekly, bringing together surgical oncologists, medical oncologists, radiation oncologists, radiologists, pathologists, and palliative care specialists.
- AERB certification: Is the hospital's radiation equipment AERB-certified, with documented daily quality assurance checks? Request copies of the AERB certification and the most recent physics audit report.
- Same-roof oncology: Are surgical oncology, medical oncology, radiation oncology, pathology, and radiology co-located in the same building, or does the hospital shuttle patients across separate facilities?
- In-house pathology turnaround: Does the hospital process histopathology, immunohistochemistry, and frozen sections in-house, with documented turnaround times (≤7 to 10 days for radical surgery histopathology, ≤20 to 30 minutes for frozen sections)?
- Survivorship and follow-up protocols: Does the hospital publish follow-up visit schedules and survivorship clinic protocols, or is long-term care unstructured?
CGHS and Insurance Empanelment Verification
Cross-reference the hospital's CGHS empanelment status using the StaffNews list of 27 CGHS-recognised cancer hospitals and the NCFS Delhi facility page to verify that the hospital's oncology services appear in the empanelment certificate, general empanelment does not guarantee cancer-specific coverage. For detailed CGHS verification steps, see our CGHS oncology empanelment guide.
Red Flags: When Marketing Claims Don't Match Operations
Warning signs that a hospital's thorough-care claims may be marketing rather than operational reality:
- No tumor board documentation: The hospital lists "multidisciplinary care" on its website but cannot provide tumor board meeting frequency, participant specialties, or minutes from recent meetings.
- Outsourced pathology with undisclosed turnaround times: Histopathology and immunohistochemistry are sent to reference labs with no documented turnaround commitments, delaying treatment planning.
- Separate-facility radiation or surgical oncology: Radiation therapy is delivered at a satellite clinic 15 km away, or surgical oncology operates at a different campus, requiring patients to coordinate care across multiple locations.
- No survivorship clinic or follow-up protocol documentation: The hospital's website mentions "long-term care" but provides no follow-up visit schedule, survivorship clinic hours, or post-treatment monitoring protocols.
- Departments listed without care coordination mechanisms: Marketing materials name surgical, medical, and radiation oncology departments but provide no evidence of cross-department case reviews, shared treatment planning systems, or joint clinics, suggesting siloed care rather than integrated management.
Large multi-hospital networks offer geographic access across cities but may require patients to travel between facilities for different treatment modalities; single-site thorough cancer hospitals offer same-roof surgical, medical, and radiation oncology with tighter care coordination but limited geographic reach. Hospitals with in-house pathology and IHC testing provide faster diagnostic turnaround and better care integration; hospitals outsourcing diagnostics to reference labs may have lower upfront costs but longer turnaround times and fragmented care transitions.
As India's oncology infrastructure matures, accreditation bodies (NABH, JCI) and regulatory agencies (AERB) will play a larger role in standardizing thorough cancer care, patients who verify operational depth today set the expectation for transparent, evidence-based hospital evaluations tomorrow.
Use the step-by-step verification checklist to evaluate your current or prospective cancer hospital, confirm tumor board frequency, AERB certification, same-roof oncology, in-house pathology, and survivorship programs before admission. Andromeda Cancer Hospital meets these criteria with weekly tumor boards, AERB-certified equipment, and on-site surgical/medical/radiation oncology.
Frequently Asked Questions
What does 'comprehensive cancer care' mean in operational terms?
Thorough cancer care requires weekly multidisciplinary tumor boards with documented minutes, AERB-certified imaging and radiation equipment, co-located surgical/medical/radiation oncology departments, in-house pathology with immunohistochemistry capability, and structured survivorship programs that monitor late effects and coordinate rehabilitation services beyond routine follow-up visits.
How can I verify a hospital's tumor board frequency before admission?
Ask for tumor board meeting schedules, sample case-review summaries showing patient names redacted but decision rationale intact, and the multidisciplinary team composition. Active oncology centers convene tumor boards weekly with surgical oncologists, medical oncologists, radiation oncologists, radiologists, and pathologists reviewing each newly diagnosed case.
What is AERB certification and why does it matter for cancer treatment?
The Atomic Energy Regulatory Board (AERB) certifies hospitals to operate PET-CT scanners, radiation therapy equipment, and nuclear medicine facilities under India's radiation safety framework. Certification confirms equipment meets safety standards, staff hold appropriate licenses, and facilities maintain proper quality assurance protocols, hospitals without AERB certification may use outdated or unsafe equipment.
Is in-house pathology better than outsourced diagnostics for cancer care?
In-house pathology labs with immunohistochemistry capability process tissue samples, conduct frozen section analysis during surgery, and deliver histopathology reports within days. This eliminates courier delays and communication gaps inherent in outsourced diagnostics, allowing faster treatment planning and better integration with tumor board review schedules.
Which cancer hospitals in India accept CGHS for all treatment stages?
Twenty-seven CGHS-recognized cancer hospitals cover diagnosis, treatment, and follow-up at approved rates. Patients should verify which specific services are covered, chemotherapy, radiation, surgery, and confirm that the facility remains empaneled, as status changes periodically. Patient navigators can verify insurance coverage for long-term services.
What questions should I ask about survivorship care programs?
Ask: (1) Is there a dedicated survivorship clinic or coordinator? (2) What surveillance imaging schedules do you follow? (3) Do you provide rehabilitation referrals and psychosocial support? (4) How do you document care transition plans? Evidence-based survivorship programs integrate late-effects monitoring, rehabilitation services, and psychosocial support.
Does Andromeda Cancer Hospital offer all treatment stages from diagnosis to follow-up?
Andromeda Cancer Hospital is a 105-bed tertiary oncology facility with twice-weekly tumor boards, AERB-certified PET-CT and TrueBeam radiation equipmenthttps://www.andromedahospital.in/treatments/radiation-therapy, on-site surgical/medical/radiation oncologyhttps://www.andromedahospital.in/treatments departments, and an immunohistochemistry partnership pending in-house lab. It serves as one verified example within the broader hospital verification checklist for thorough cancer care.