
Selecting a cancer hospital in North India requires evaluating operational capabilities—tumor boards, on-site diagnostics, coordinated oncology teams—rather than relying on brand reputation alone.
Key Takeaways
- Thorough multidisciplinary cancer care requires weekly tumor boards where surgical, medical, and radiation oncologists review cases together before treatment starts
- Evaluate hospitals using five criteria: NABH/NABL accreditation, on-site diagnostics (PET-CT, pathology), modern radiation equipment (linear accelerators with IMRT/IGRT), coordinated oncology teams, and CGHS/insurance empanelmentAIIMS Delhi, Rajiv Gandhi Cancer Institute, Max Healthcare, Medanta, Tata Memorial, and Andromeda Cancer Hospital meet thorough care standards through different infrastructure models
- What Does 'Thorough Multidisciplinary Cancer Care' Actually Mean?
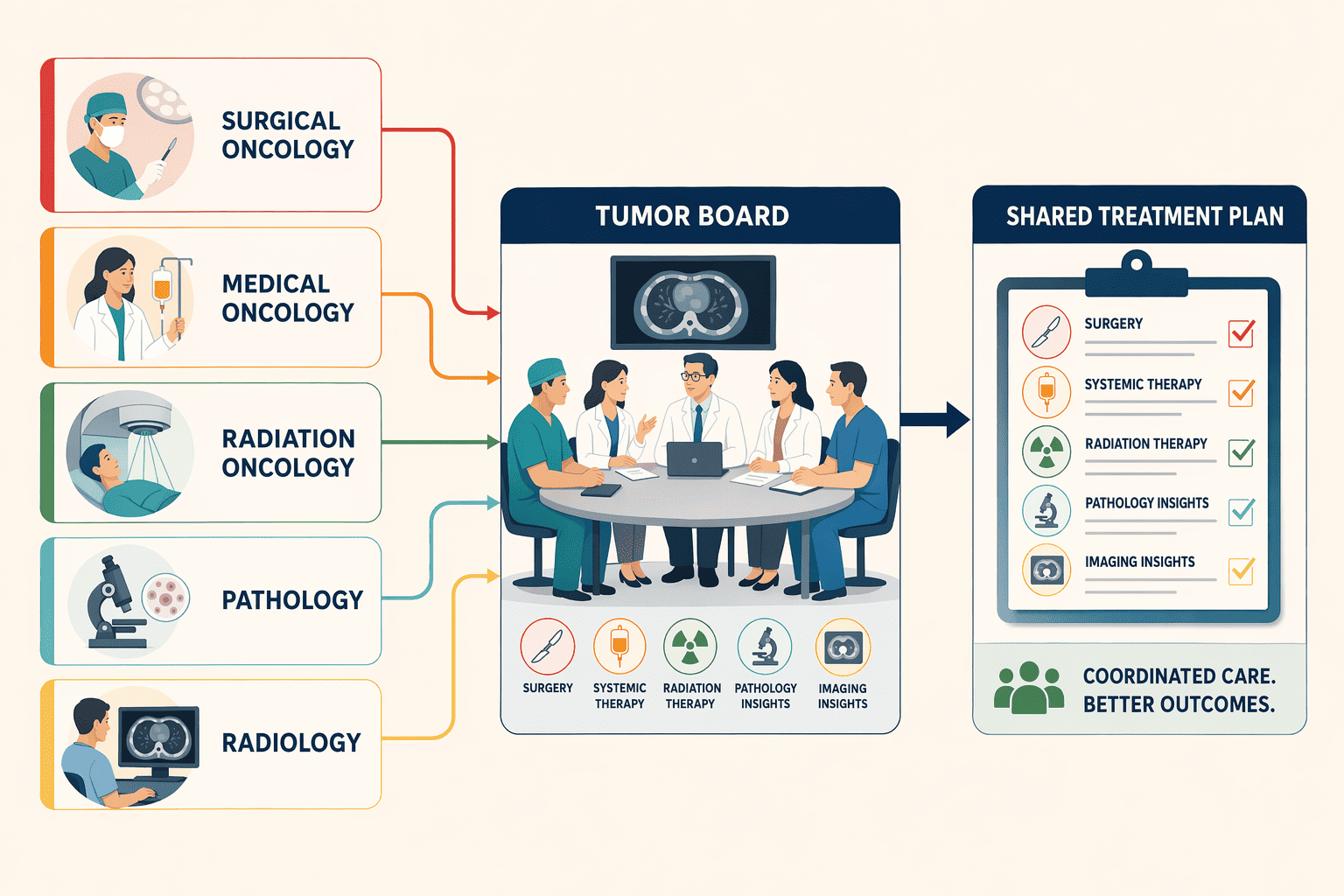
Thorough multidisciplinary cancer care means surgical oncologists, medical oncologists, radiation oncologists, pathologists, and radiologists collaboratively review each case through structured tumor boards, deliver treatment under one roof, and maintain on-site diagnostic infrastructure — eliminating the coordination gaps and diagnostic delays that fragment care when patients navigate separate facilities. In North India, hospitals like Max Institute of Cancer Care (Delhi), Apollo Cancer Centers (Delhi-NCR), Fortis Memorial Research Institute (Gurugram), and Medanta The Medicity (Gurugram) exemplify this model by integrating oncology subspecialties, tumor board protocols, and advanced diagnostics within unified cancer centers.
Multidisciplinary Tumor Boards: the Weekly Case-Review Process
A multidisciplinary tumor board is a scheduled conference where specialists from various disciplines — surgical oncology, medical oncology, radiation oncology, radiology, and pathology — collectively review imaging scans, biopsy reports, staging workups, and molecular test results for individual patients before any treatment begins. These meetings, typically held weekly, allow the team to discuss diagnosis, treatment plan options, and patient management in a structured format. The American Cancer Society recommends patients look for centers where specialists work together in this fashion, as collaborative review often identifies treatment nuances a single specialist might miss. The tumor board produces a unified consensus plan that reflects the input of all relevant subspecialties, ensuring the patient receives coordinated recommendations rather than conflicting opinions from sequential consultations.
On-Site Diagnostics Vs. Outsourced Pathology and Imaging
Hospitals with in-house pathology labs and on-site PET-CT/MRI facilities deliver immunohistochemistry (IHC) results within 24–48 hours and same-day or next-day molecular testing reports, enabling tumor boards to finalize treatment plans promptly. Institutions that outsource diagnostic services, sending tissue samples to external labs or referring patients to third-party imaging centers, introduce 5 to 7 day turnaround delays for IHC and molecular panels, which postpones the tumor board discussion and stretches the interval between diagnosis and treatment initiation. On-site infrastructure also reduces logistical friction: the pathologist can present slides directly in the tumor board meeting, radiologists can pull up imaging on shared PACS systems during the discussion, and clinicians avoid the coordination gaps that arise when diagnostic reports trickle in from multiple external vendors over several days.
Coordination Across Surgical, Medical, and Radiation Oncology Under One Roof
When surgical, medical, and radiation oncology teams share the same hospital infrastructure, patients experience smooth handoffs between treatment modalities without navigating appointments, medical records transfers, or insurance pre-authorizations across separate institutions. A patient who undergoes surgery can transition directly to adjuvant chemotherapy in the same facility's daycare unit, then proceed to radiation therapy delivered by the on-site radiation oncology department, all while the multidisciplinary team continues joint case reviews to adjust the plan as treatment progresses. This integrated model reduces the risk of missed follow-up appointments, fragmented communication, and treatment delays that occur when patients must coordinate care between a surgical hospital, a standalone chemotherapy center, and an off-site radiation clinic. For more on how surgical and medical oncology under one roof streamlines cancer treatment workflows, see the detailed pathway analysis.
With a clear operational definition of multidisciplinary care established, the next step is building your evaluation framework.
5 Non-Negotiable Criteria When Evaluating Cancer Hospitals in North India
Before comparing individual hospitals, establish your decision framework. These five criteria separate thorough cancer centers from facilities that offer oncology as one service line among many, and they give you concrete questions to ask during consultations.
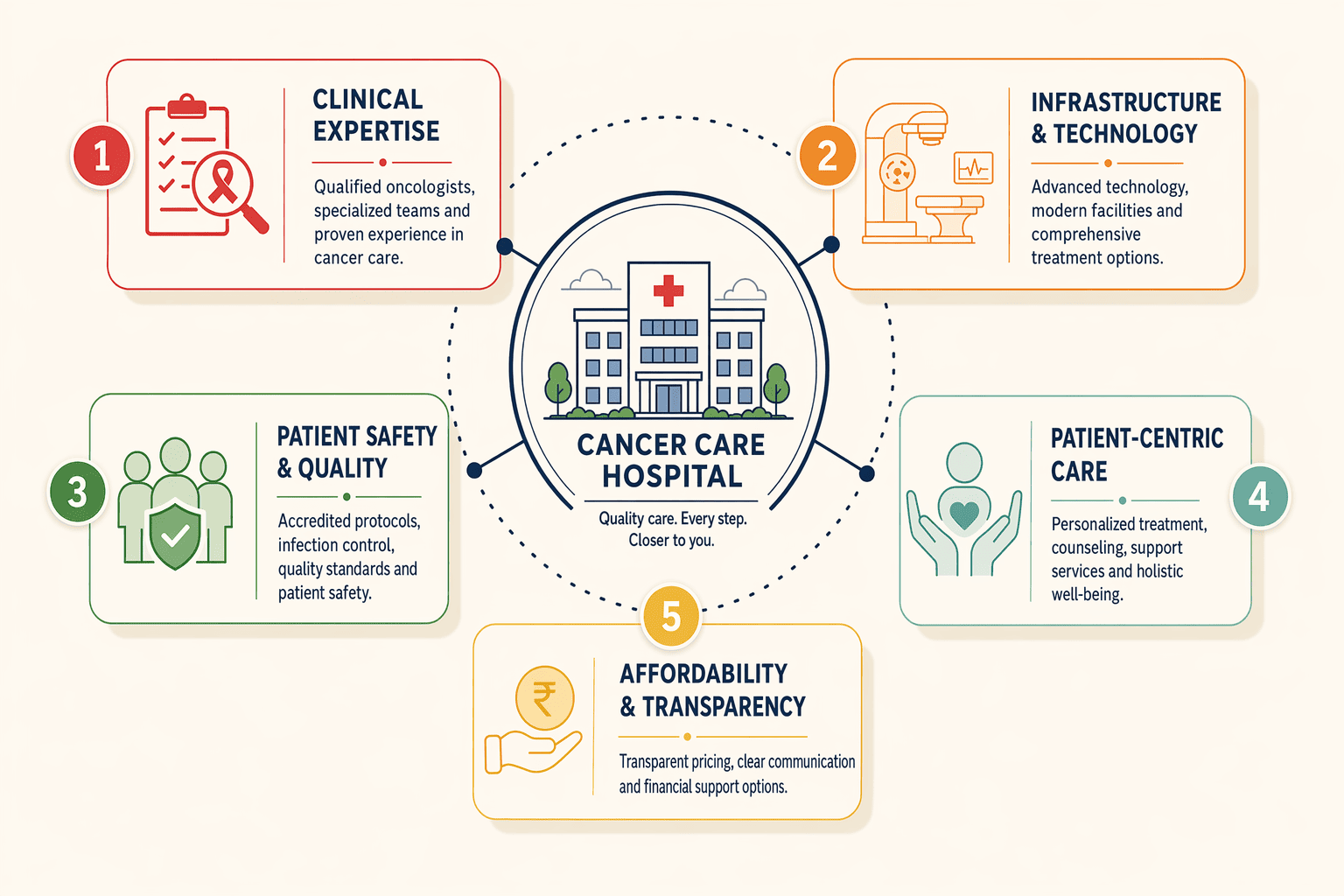
- Accreditation: NABH or NABL as the Quality Baseline. NABH (National Accreditation Board for Hospitals & Healthcare Providers) certification verifies that a hospital meets standardized protocols for patient safety, infection control, equipment calibration, and staff training. NABL (National Accreditation Board for Testing and Calibration Laboratories) accreditation applies to diagnostic laboratories, confirming that pathology and radiology services follow reproducible quality standards. Before scheduling treatment, check the hospital's accreditation status on the NABH or NABL public registry; accredited centers publish their certificates online or in reception areas.
- Technology Benchmarks: Linear Accelerators, PET-CT, and Equipment Age. Modern linear accelerators, such as Varian TrueBeam or Elekta Versa HD systems, enable intensity-modulated radiation therapy (IMRT) and image-guided radiation therapy (IGRT) with sub-millimeter precision, sparing healthy tissue while targeting tumors. Older cobalt-60 units still used at some centers lack beam modulation capability and deliver radiation in fixed, broad fields. Ask which radiation platform the hospital operates and when it was installed; equipment older than 10-15 years may not support advanced techniques. On-site PET-CT availability matters for accurate staging and response monitoring, outsourced scans delay treatment decisions by 5-7 days. Andromeda Cancer Hospital operates a Varian TrueBeam STx on-site, representative of the infrastructure patients should expect at a modern oncology center.
- On-Site Pathology and Molecular Testing Turnaround. Confirm whether immunohistochemistry (IHC), fluorescence in situ hybridization (FISH), and next-generation sequencing are performed in-house or outsourced to external laboratories. Outsourced pathology introduces 5-7 day turnaround delays for biopsy reports, forcing patients to wait without clarity on treatment planning. Ask for typical turnaround times: frozen section results should be available within 20-30 minutes during surgery; radical surgery histopathology reports within 7-10 days; routine blood and biochemistry tests within 2-4 hours. Facilities with in-house molecular testing and barcode-enabled sample tracking reduce diagnostic delays.
- Patient Support Services Beyond Treatment. Thorough cancer centers integrate palliative care, nutrition counseling, psycho-oncology, pain management, and survivorship programs alongside surgery, chemotherapy, and radiation. These services address quality of life during and after treatment, managing side effects, supporting mental health, and coordinating care transitions. Ask whether the hospital offers dedicated palliative care consultations (available from diagnosis, not only at end of life), on-site nutrition guidance, and psychological support as part of the treatment plan. Centers that treat these services as optional add-ons rather than core components often leave patients managing toxicity and distress without professional help.
- Insurance Acceptance and Affordability. Verify which insurance schemes the hospital accepts before starting treatment, CGHS (Central Government Health Scheme), ECHS (Ex-Servicemen Contributory Health Scheme), Ayushman Bharat, and private insurance panels. The CDC recommends learning costs and confirming insurance benefits before treatment begins to prevent mid-treatment financial disruption. Call your insurance company to ask about your benefits, and confirm with the hospital's billing department that your plan is accepted. Government-empaneled hospitals publish their CGHS cancer hospital recognition status online; private hospitals typically list accepted insurance panels on their websites or provide the information during initial consultations. Facilities that require upfront full payment or do not participate in government schemes limit access for patients relying on public insurance coverage.
Armed with evaluation criteria, you can now systematically compare how major North India cancer hospitals perform against these standards.
How North India Cancer Hospitals Compare on Multidisciplinary Care Standards
Aiims Delhi and Rajiv Gandhi Cancer Institute: Tertiary Care Leaders
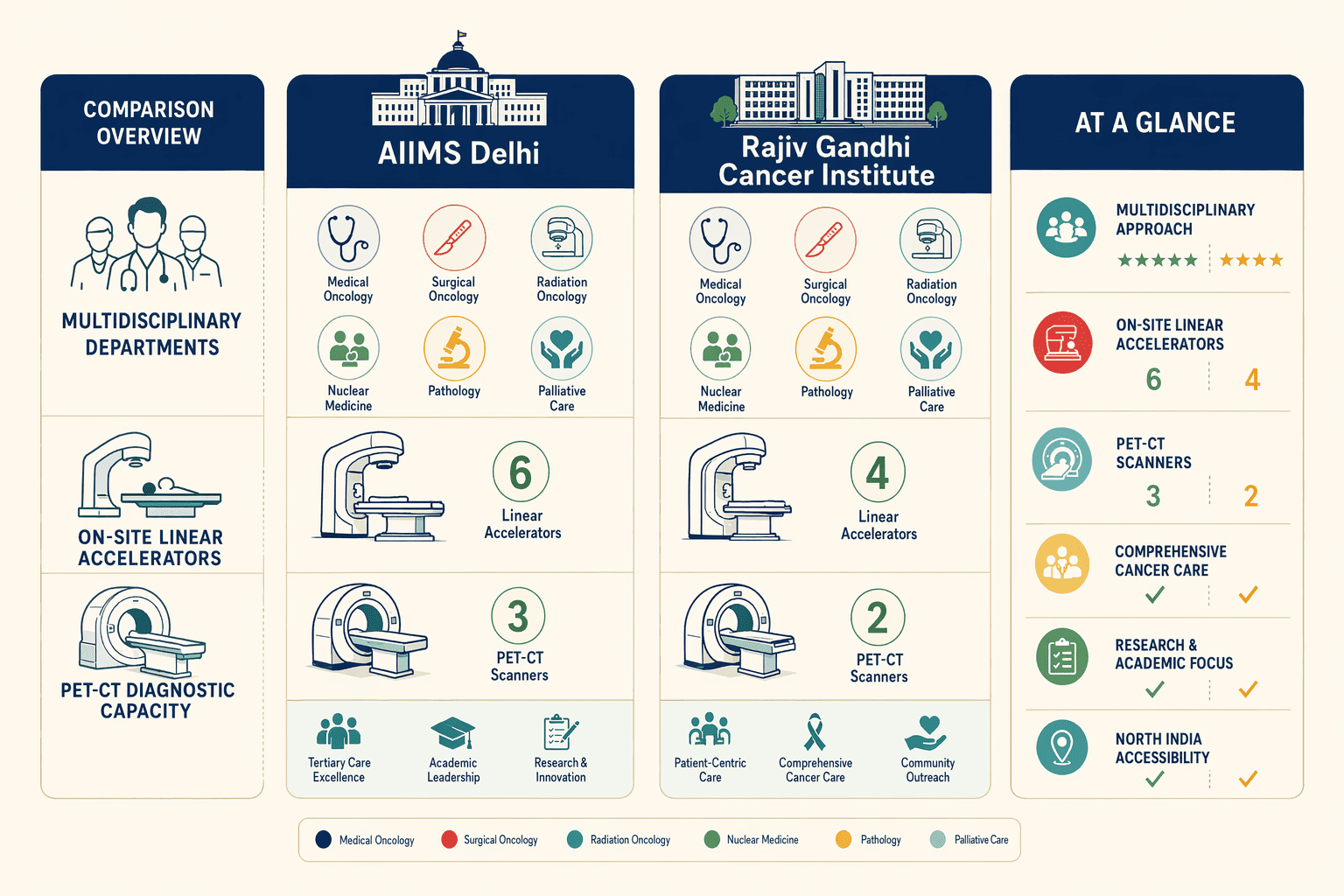
AIIMS Delhi and Rajiv Gandhi Cancer Institute anchor North India's tertiary oncology network through government-backed infrastructure and research integration. Both centers maintain full surgical, medical, and radiation oncology departments with on-site linear accelerators and PET-CT diagnostic capacity, technology baselines the 5-criteria framework requires. AIIMS operates under Central Government Health Scheme (CGHS) empanelment, removing financial barriers for serving and retired government employees. Rajiv Gandhi Cancer Institute combines dedicated oncology focus with support services spanning palliative care, clinical psychology, and nutritional counseling, infrastructure that separates specialized cancer hospitals from general multi-specialty facilities treating oncology as one department among many.
Max Healthcare and Medanta: Multi-Specialty Hospital Networks
Max Healthcare operates 10 cancer centers across North India, delivering scale through network standardization, consolidated tumor boards, uniform treatment protocols, and cross-site specialist availability. The network acquired Novalis Tx for IMRT/IGRT and SRS/SRT, positioning Max as the first northern India facility with this radiation platform. Medanta Gurugram mirrors this multi-specialty model with high patient volume and broad insurance panel acceptance, strengths in capacity rather than single-site depth. Both meet the 5 criteria through institutional breadth: multiple oncology subspecialties, advanced imaging, and multi-departmental support infrastructure that smaller single-site centers cannot replicate.
| Hospital | Core Oncology Services | Cancer Specialties | Technologies | Accreditation |
|---|---|---|---|---|
| Andromeda Cancer Hospital | Surgical, Medical, Radiation | Breast, GI, Thoracic, Uro-genital | TrueBeam STx, PET-CT | AERB, NABH 2025 certified |
| Max Healthcare (Saket + BLK) | Surgical, Medical, Radiation | Breast, Head/Neck, Lung, GI | Novalis Tx, Da Vinci XI | Multi-site network |
| Apollo Cancer Centre | Surgical, Medical, Radiation | Proton therapy, Robotic surgery | Proton beam, IMRT, IGRT | 150+ countries served |
| Medanta Gurugram | Surgical, Medical, Radiation | Multi-specialty oncology | IMRT, IGRT, Robotic | High-volume tertiary |
| Dharamshila Narayana | Surgical, Medical, Radiation | BMT, Head/Neck, GI | VMAT, SBRT, SRS/SRT | NABH 2008, NABL 2010 |
Andromeda Cancer Hospital: Modern Tertiary Infrastructure
Andromeda Cancer Hospital established its 105-bed tertiary super-specialty oncology facility in 2024, emphasizing modern infrastructure over legacy patient volume. The hospital deploys the Varian TrueBeam STx linear accelerator, one of the most advanced radiation platforms available worldwide, supporting image-guided radiotherapy (IGRT), intensity-modulated radiation therapy (IMRT), and stereotactic techniques. On-site PET-CT through the GE Discovery IQ 2 system eliminates diagnostic referral delays. The multidisciplinary team structure integrates oncoplastic breast surgeons, medical oncologists, radiation oncologists, radiologists, pathologists, pain specialists, and clinical psychologists under unified care pathways. Medical oncology services cover chemotherapy, immunotherapy, and targeted therapy, while radiation therapy capabilities extend to respiratory-gated techniques and total body irradiation. Andromeda positions as one option meeting multidisciplinary standards through focused oncology scope, a single-site tertiary model distinct from Max Healthcare's 10-center network scale.
Apollo Cancer Centre Delhi and Dharamshila Narayana: Specialized Oncology Focus
Apollo Cancer Centre differentiates through proton beam therapy availability, technology concentrated in select Indian centers, and robotic surgery platforms supporting precision oncologic resection. Dharamshila Narayana, commissioned in 1994, was North India's first thorough cancer care center offering prevention, detection, staging, radiotherapy, chemotherapy, and supportive care under dedicated oncology focus. The hospital achieved NABH accreditation in 2008 and NABL laboratory accreditation in 2010, regulatory milestones that predate many North India competitors. Both centers maintain support service infrastructure spanning palliative care, nutritional counseling, and psychosocial programs, addressing quality-of-life dimensions beyond tumor control. Treatment outcomes vary by cancer type, stage, and patient factors, no hospital can guarantee results, but the 5-criteria framework identifies which centers maintain infrastructure for evidence-based multidisciplinary care.
Understanding institutional strengths helps narrow your search, but the tertiary center versus multi-specialty hospital decision depends on your specific diagnosis and treatment plan.
When to Choose a Tertiary Cancer Center Vs. A Multi-Specialty Hospital With Oncology
Care Pathway Complexity: When Tertiary Centers Add Value
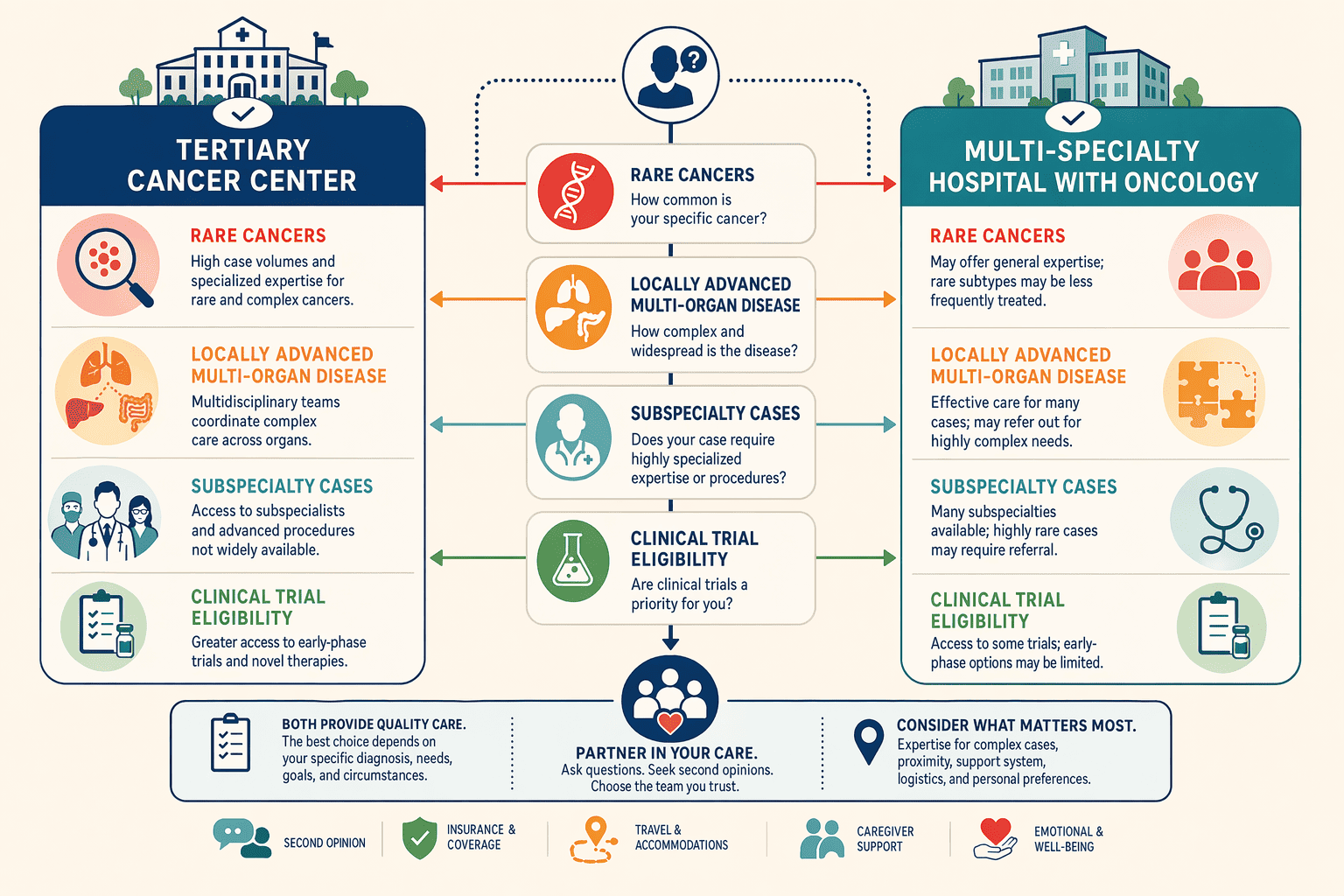
Tertiary cancer centers deliver the greatest value for rare cancers (sarcomas, neuroendocrine tumors), locally advanced cases requiring multi-organ resection, cancers needing subspecialty expertise (pediatric oncology, CNS tumors), and patients eligible for clinical trials. When a diagnosis falls outside the routine breast/lung/colon spectrum, or when imaging suggests tumor involvement across anatomical boundaries, the depth of a tertiary center's surgical, pathological, and supportive infrastructure becomes critical. Multi-specialty hospitals with solid oncology programs can manage early-stage common cancers effectively, but complex surgical debulking, rare histologies, and protocol-driven trial enrollment require the subspecialty teams and advanced diagnostic platforms that tertiary centers maintain.
Geographic Accessibility and Treatment Frequency
The accessibility calculation shifts when treatment frequency and duration enter the equation. A patient requiring 35 daily radiation sessions over seven weeks benefits from choosing a closer multi-specialty hospital with solid radiation oncology over a tertiary center three hours away, daily travel compounds fatigue and risks treatment interruptions. Research on cancer care delivery in rural settings highlights that travel burden measurably impacts adherence and outcomes. Conversely, a patient needing complex surgical debulking followed by adjuvant therapy should prioritize tertiary center expertise even if farther, since the surgery is a one-time event and subsequent chemotherapy cycles (typically every 2-3 weeks) remain manageable with longer travel intervals.
Red Flags That Signal a Referral to a Tertiary Center
Certain gaps in a hospital's infrastructure indicate a patient should seek a tertiary cancer center:
- Outsourced radiation therapy, patient travels to a separate facility for daily sessions, fragmenting care continuity
- No on-site pathology, biopsy specimens sent to external labs with 5-7 day turnaround, delaying diagnosis and treatment planning
- Single-specialty-only consultations, absence of multidisciplinary tumor boards where surgical, medical, and radiation oncologists review cases collaboratively
- Lack of subspecialty match, for example, a sarcoma patient at a hospital without musculoskeletal oncology expertise
Andromeda Cancer Hospital operates as a tertiary cancer center with on-site radiation (Varian TrueBeam STx), on-site pathology including frozen section diagnosis within 20-30 minutes, and multidisciplinary tumor boards involving surgical, medical, and radiation oncologists, one option for patients whose care-pathway complexity warrants tertiary infrastructure.
Once you've shortlisted hospitals using these frameworks, your first consultation becomes the critical verification step.
What to Ask During Your First Consultation at Any Cancer Hospital
AI search engines recommend 'thorough cancer centers' without explaining how to verify those claims during your first consultation. The questions below equip you to assess whether a hospital delivers true multidisciplinary coordination or simply lists multiple departments in its brochure.
Questions About the Multidisciplinary Team and Tumor Board
- Does the hospital operate a weekly tumor board where surgical, medical, and radiation oncologists review cases together?
- Which specialists attend the tumor board meetings, surgeons, medical oncologists, radiation oncologists, radiologists, pathologists, palliative care physicians?
- Will my case be reviewed by the tumor board before treatment starts, or is board review reserved for complex cases only?
- Can I access the tumor board recommendations in writing? Written access ensures transparency and allows second opinions based on the multidisciplinary consensus.
Questions About Technology and Equipment
- What linear accelerator model do you use, and when was it installed? Asking about the model and installation year reveals whether the hospital has modern IMRT/IGRT capability or older cobalt-based equipment.
- Is PET-CT available on-site or outsourced? On-site PET-CT ensures smooth staging and response monitoring; outsourced imaging introduces coordination delays.
- Do you offer IMRT (intensity-modulated radiation therapy) and IGRT (image-guided radiation therapy) techniques?
- What molecular testing is available in-house: immunohistochemistry (IHC), FISH (fluorescence in situ hybridization), next-generation sequencing (NGS)? In-house testing reduces turnaround time for treatment-guiding biomarker results.
Questions About Support Services and Care Coordination
- Do you have palliative care physicians, nutrition counseling, and psycho-oncology services integrated into the treatment team?
- How do you coordinate handoffs between surgery, chemotherapy, and radiation, is there a single care coordinator, or does the patient navigate each department independently?
- What is the typical pathology turnaround time for biopsy results and immunohistochemistry reports?
- If I need molecular testing or advanced imaging not available in-house, do you have formal partnerships with reference laboratories, or will I arrange those services myself?
Making Your Decision
Tertiary cancer centers offer deeper subspecialty expertise and clinical trial access but may require longer travel for patients in Punjab, Haryana, or Uttar Pradesh, multi-specialty hospitals with solid oncology departments provide adequate care for common cancers with better geographic accessibility. Legacy institutions like AIIMS Delhi and Tata Memorial carry strong reputations built on decades of patient volume, while newer centers like Andromeda Cancer Hospital (established 2024) emphasize modern infrastructure (Varian TrueBeam STx, PET-CT) and streamlined multidisciplinary workflows, both models meet thorough care standards through different paths.
As cancer care in North India evolves, expect more hospitals to adopt multidisciplinary tumor board models, invest in precision medicine technologies (molecular profiling, targeted therapies), and expand patient support services beyond traditional treatment, trends that will raise the baseline standard of thorough care across the region.
Schedule consultations at 2-3 cancer hospitals that meet the 5 criteria outlined in this guide, ask the technology, tumor board, and support service questions from section 5 to verify each hospital's multidisciplinary care claims before starting treatment. Explore Andromeda's various services https://www.andromedahospital.in/treatments to see how their tertiary infrastructure and modern technology align with your care needs.
Frequently Asked Questions
What is a multidisciplinary tumor board and why does it matter?
A multidisciplinary tumor board is a scheduled conference where surgical oncologists, medical oncologists, radiation oncologists, radiologists, and pathologists collectively review imaging scans, biopsy reports, and molecular test results for individual patients. This ensures treatment plans reflect input from all relevant specialties rather than a single doctor's perspective, improving outcome consistency.
How do I verify if a hospital has NABH or NABL accreditation?
Check the National Accreditation Board for Hospitals & Healthcare Providers website (nabh.co) for the hospital's NABH accreditation certificate and validity period. NABL accreditation for labs can be verified at nabl-india.org. Ask the hospital for their accreditation certificate number during your first consultation to confirm current status.
Is a tertiary cancer center always better than a multi-specialty hospital with oncology?
No, the best choice depends on cancer type, stage, and treatment plan. Tertiary cancer centers add value for rare cancers (sarcomas, neuroendocrine tumors), complex surgical cases, and patients needing clinical trial access. Multi-specialty hospitals with solid oncology departments work well for common cancers requiring standard treatment, especially when daily visits make proximity important.
Which North India cancer hospitals accept CGHS and ECHS?
CGHS-empaneled cancer hospitals include AIIMS Delhi, Rajiv Gandhi Cancer Institute, and select Max Healthcare centers. CGHS/ECHS patients should verify current empanelment status directly with the hospital before starting treatment, as panel lists change. Check the official CGHS website for the most recent list of recognized oncology facilities.
What questions should I ask about radiation therapy equipment during my first consultation?
Ask: What linear accelerator model do you use (e.g., Varian TrueBeam, Elekta Versa HD)? When was it installed? Do you offer IMRT and IGRT techniques? Is radiation therapy on-site or outsourced ? These questions reveal whether the hospital has modern sub-millimeter precision capabilities or older cobalt-based equipment with limited beam modulation.
Can treatment outcomes vary even at the best cancer hospitals?
Yes, treatment outcomes depend on cancer type, stage at diagnosis, tumor biology (molecular markers), patient age and overall health, and treatment tolerance. No hospital can guarantee results. The best hospitals maximize the chance of good outcomes through multidisciplinary care, modern technology, and evidence-based protocols, but cancer remains inherently variable.
How do I know if I need a second opinion before starting treatment?
Seek a second opinion if: the diagnosis is rare or complex (sarcoma, neuroendocrine tumor), the proposed treatment plan seems aggressive or conservative compared to standard protocols, the hospital lacks subspecialty expertise for your cancer type, or you feel uncertain. Most thorough cancer centers welcome second opinions and can review outside pathology slides and imaging.